Chen Yu-Tong, Seeruttun Sharvesh Raj, Wu Xiang-Yuan, Wang Zi-Xian
Department of Medical Oncology, Third Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Department of Surgical Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Front Oncol. 2019 Dec 17;9:1432. doi: 10.3389/fonc.2019.01432. eCollection 2019.
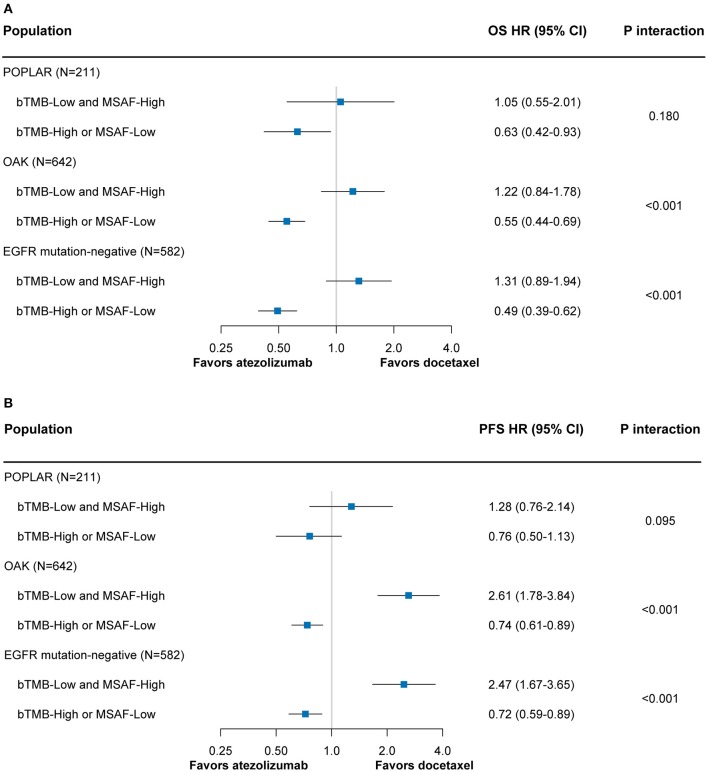
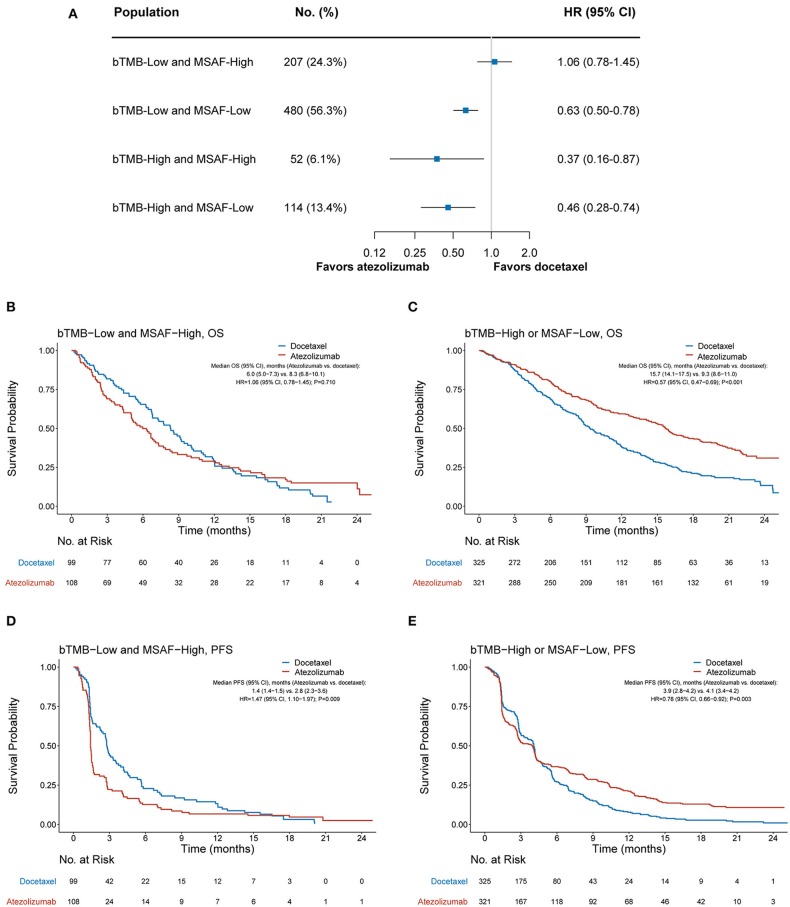
Blood-based tumor mutational burden (bTMB) was recently found to be suboptimal in predicting overall survival (OS) benefits of atezolizumab over docetaxel among patients with advanced non-small cell lung cancer (NSCLC). The maximum somatic allele frequency (MSAF) is an indicator of the proportion of tumor-derived plasma DNA, which could affect the concordance between bTMB and tissue-based TMB. Therefore, we aimed to evaluate the utility of MSAF, alone or in combination with bTMB, to identify NSCLC patients with or without survival benefit from atezolizumab over docetaxel. We analyzed the individual patient-level data from the randomized POPLAR and OAK studies. The bTMB and MSAF were derived from the pre-treatment blood-based genomic data. In both the bTMB-high (i.e., bTMB ≥ 13) and bTMB-low subgroups, atezolizumab significantly improved OS compared with docetaxel (hazard ratio [HR] = 0.43 [95% CI, 0.29-0.65], < 0.001 and HR = 0.73 [95% CI, 0.61-0.87], < 0.001, respectively). Among patients with a low MSAF (i.e., MSAF < 10.3%), OS significantly favored atezolizumab (HR = 0.59 [95% CI, 0.48-0.72], < 0.001), whereas OS with atezolizumab was similar to that with docetaxel in the MSAF-high subgroup (HR = 0.91 [95% CI, 0.68-1.20], = 0.500; interaction test = 0.017). Among patients from the bTMB-low and MSAF-high subgroup, OS was numerically worse with atezolizumab than with docetaxel (HR = 1.06 [95% CI, 0.78-1.45], = 0.710); in contrast, OS was significantly improved with atezolizumab compared with docetaxel in those with either a high bTMB or low MSAF (HR = 0.57 [95% CI, 0.47-0.69], < 0.001; interaction test < 0.001). Consistent findings were obtained for progression-free survival data. MSAF alone or in combination with bTMB can effectively distinguish patients with or without survival benefit from atezolizumab compared with docetaxel. MSAF and the combined bTMB-MSAF classification may become practical predictive markers for atezolizumab in advanced NSCLC.
最近发现,在晚期非小细胞肺癌(NSCLC)患者中,基于血液的肿瘤突变负荷(bTMB)在预测阿特珠单抗对比多西他赛的总生存期(OS)获益方面表现欠佳。最大体细胞等位基因频率(MSAF)是肿瘤来源的血浆DNA比例的一个指标,它可能会影响bTMB与基于组织的TMB之间的一致性。因此,我们旨在评估MSAF单独或与bTMB联合使用,以识别接受阿特珠单抗对比多西他赛治疗是否有生存获益的NSCLC患者。我们分析了来自随机化的POPLAR和OAK研究的个体患者水平数据。bTMB和MSAF来自治疗前基于血液的基因组数据。在bTMB高(即bTMB≥13)和bTMB低亚组中,与多西他赛相比,阿特珠单抗均显著改善了OS(风险比[HR]=0.43[95%CI,0.29 - 0.65],P<0.001和HR = 0.73[95%CI,0.61 - 0.87],P<0.001)。在MSAF低(即MSAF<10.3%)的患者中,OS显著有利于阿特珠单抗(HR = 0.59[95%CI,0.48 - 0.72],P<0.001),而在MSAF高亚组中,阿特珠单抗的OS与多西他赛相似(HR = 0.91[95%CI,0.68 - 1.20],P = 0.500;交互检验P = 0.017)。在bTMB低且MSAF高亚组的患者中,阿特珠单抗的OS在数值上比多西他赛差(HR = 1.06[95%CI,0.78 - 1.45],P = 0.710);相反,在bTMB高或MSAF低的患者中,与多西他赛相比,阿特珠单抗显著改善了OS(HR = 0.57[95%CI,0.47 - 0.69],P<0.001;交互检验P<0.001)。无进展生存期数据也得到了一致的结果。单独的MSAF或与bTMB联合使用可以有效区分接受阿特珠单抗对比多西他赛治疗是否有生存获益的患者。MSAF以及联合的bTMB - MSAF分类可能成为晚期NSCLC中阿特珠单抗的实用预测标志物。