Department of Radiology, The Affiliated BenQ Hospital of Nanjing Medical University, Nanjing, China.
Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University School of Medicine, Haidian District, Beijing, 100084, China.
J Cardiovasc Magn Reson. 2020 Jan 13;22(1):4. doi: 10.1186/s12968-019-0596-6.
It is still unknown that whether co-existing intracranial stenosis and extracranial carotid vulnerable plaques have higher predictive value for subsequent vascular events. This study aimed to determine the relationship between co-existing extracranial carotid vulnerable plaques and intracranial stenosis and subsequent vascular events utilizing cardiovascular magnetic resonance (CMR) vessel wall imaging.
Patients who had recent cerebrovascular symptoms in anterior circulation (< 2 weeks) were consecutively enrolled and underwent multi-contrast CMR vessel wall imaging for extracranial carotid arteries and 3D time-of flight CMR angiography for intracranial arteries at baseline. After baseline examination, all patients were followed-up for at least 1 year to determined recurrence of vascular events. The co-existing cerebrovascular atherosclerosis was defined as presence of both intracranial artery stenosis and at least one the following measures of extracranial artery atherosclerosis: plaque, calcification, lipid-rich necrotic core (LRNC), or intraplaque hemorrhage. Univariate and multivariate Cox regressions were used to calculate the hazard ratio (HR) and corresponding 95% confidence interval (CI) of co-existing plaques in predicting subsequent vascular events.
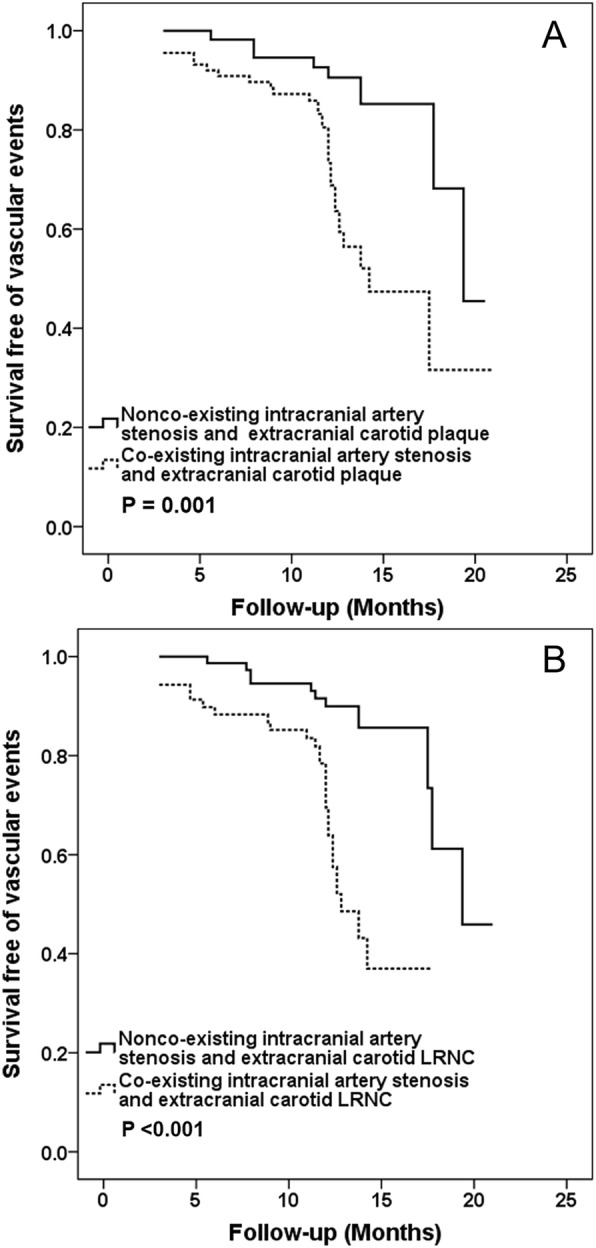
In total, 150 patients (mean age: 61.8 ± 11.9 years; 109 males) were recruited. During the median follow-up time of 12.1 months, 41 (27.3%) patients experienced vascular events. Co-existing intracranial artery stenosis and extracranial carotid plaque (HR, 3.57; 95% CI, 1.63-7.82; P = 0.001) and co-existing intracranial artery stenosis and extracranial carotid LRNC (HR, 4.47; 95% CI, 2.15-9.27; P < 0.001) were significantly associated with subsequent vascular events, respectively. After adjusted for confounding factors and carotid stenosis, these associations remained statistically significant (HR, 5.12; 95% CI, 1.36-19.24; P = 0.016 and HR, 8.12; 95% CI, 2.41-27.31; P = 0.001, respectively).
The co-existing cerebrovascular atherosclerotic diseases, particularly co-existing carotid lipid-rich necrotic core and intracranial stenosis, are independent predictors for subsequent vascular events.
目前尚不清楚同时存在颅内狭窄和颅外颈动脉易损斑块是否对后续血管事件具有更高的预测价值。本研究旨在利用心血管磁共振(CMR)血管壁成像来确定颅外颈动脉易损斑块与颅内狭窄并存与后续血管事件之间的关系。
连续纳入近期在前循环(<2 周)出现脑血管症状的患者,并在基线时进行多对比 CMR 血管壁成像以评估颅外颈动脉,以及 3D 时间飞跃 CMR 血管造影以评估颅内动脉。在基线检查后,所有患者均至少随访 1 年以确定血管事件的复发情况。共存性脑血管粥样硬化定义为同时存在颅内动脉狭窄和以下至少一项颅外动脉粥样硬化措施:斑块、钙化、富含脂质的坏死核心(LRNC)或斑块内出血。采用单变量和多变量 Cox 回归计算共存斑块预测后续血管事件的风险比(HR)及其相应的 95%置信区间(CI)。
共纳入 150 例患者(平均年龄:61.8±11.9 岁;109 例男性)。在中位随访时间 12.1 个月期间,41 例(27.3%)患者发生了血管事件。同时存在颅内动脉狭窄和颅外颈动脉斑块(HR,3.57;95%CI,1.63-7.82;P=0.001)和同时存在颅内动脉狭窄和颅外颈动脉 LRNC(HR,4.47;95%CI,2.15-9.27;P<0.001)与随后的血管事件显著相关。在校正混杂因素和颈动脉狭窄后,这些关联仍然具有统计学意义(HR,5.12;95%CI,1.36-19.24;P=0.016 和 HR,8.12;95%CI,2.41-27.31;P=0.001)。
共存性脑血管粥样硬化性疾病,特别是同时存在颈动脉富含脂质的坏死核心和颅内狭窄,是后续血管事件的独立预测因素。