Department of Medical Microbiology and Infectious Diseases, Erasmus University Medical Center, Rotterdam, The Netherlands.
Department of Hospital Pharmacy, Erasmus University Medical Center, Rotterdam, The Netherlands.
Clin Pharmacokinet. 2020 Jul;59(7):885-898. doi: 10.1007/s40262-020-00859-1.
Population pharmacokinetic (popPK) models for antibiotics are used to improve dosing strategies and individualize dosing by therapeutic drug monitoring. Little is known about the differences in results of parametric versus nonparametric popPK models and their potential consequences in clinical practice. We developed both parametric and nonparametric models of imipenem using data from critically ill patients and compared their results.
Twenty-six critically ill patients treated with intravenous imipenem/cilastatin were included in this study. Median estimated glomerular filtration rate (eGFR) measured by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation was 116 mL/min/1.73 m (interquartile range 104-124) at inclusion. The usual dosing regimen was 500 mg/500 mg four times daily. On average, five imipenem levels per patient (138 levels in total) were drawn as peak, intermediate, and trough levels. Imipenem concentration-time profiles were analyzed using parametric (NONMEM 7.2) and nonparametric (Pmetrics 1.5.2) popPK software.
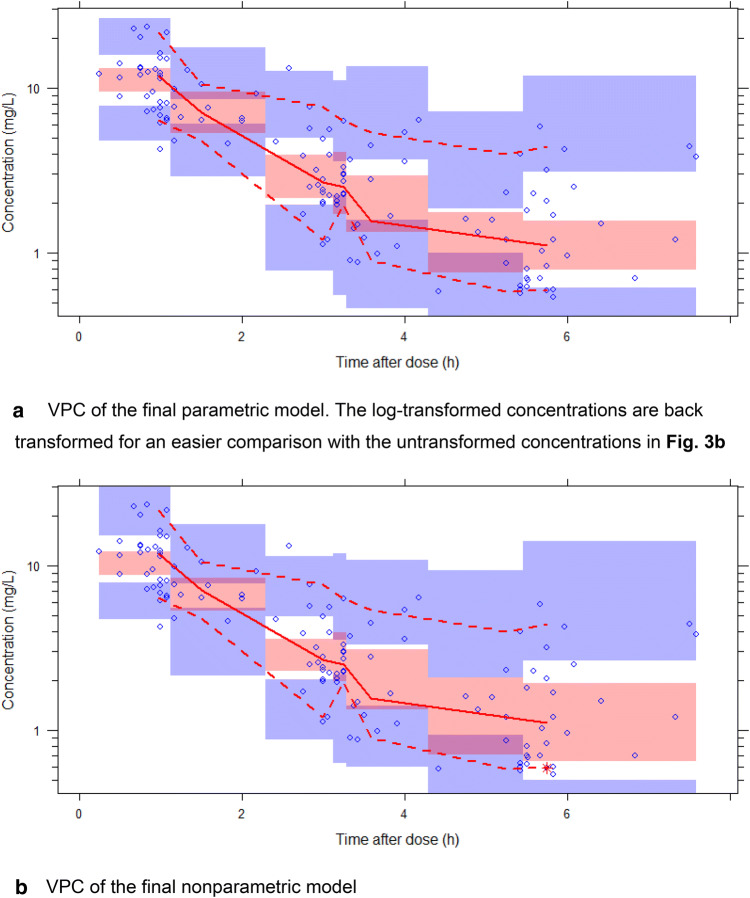
For both methods, data were best described by a model with two distribution compartments and the CKD-EPI eGFR equation unadjusted for body surface area as a covariate on the elimination rate constant (K). The parametric population parameter estimates were K 0.637 h (between-subject variability [BSV]: 19.0% coefficient of variation [CV]) and central distribution volume (V) 29.6 L (without BSV). The nonparametric values were K 0.681 h (34.0% CV) and V 31.1 L (42.6% CV).
Both models described imipenem popPK well; the parameter estimates were comparable and the included covariate was identical. However, estimated BSV was higher in the nonparametric model. This may have consequences for estimated exposure during dosing simulations and should be further investigated in simulation studies.
抗生素群体药代动力学(popPK)模型用于通过治疗药物监测来改善给药方案和实现个体化给药。对于参数法和非参数法 popPK 模型的结果差异及其在临床实践中的潜在影响,人们知之甚少。我们使用来自重症患者的数据开发了亚胺培南的参数法和非参数法模型,并对其结果进行了比较。
本研究纳入了 26 例接受静脉注射亚胺培南/西司他丁治疗的重症患者。纳入时,根据慢性肾脏病流行病学合作(CKD-EPI)方程估算的肾小球滤过率(eGFR)中位数为 116 mL/min/1.73 m (四分位间距 104-124)。常规给药方案为 500 mg/500 mg ,每日 4 次。平均每位患者抽取 5 个亚胺培南血药浓度(共 138 个浓度),分别为峰浓度、中点浓度和谷浓度。使用参数法(NONMEM 7.2)和非参数法(Pmetrics 1.5.2)popPK 软件对亚胺培南浓度-时间曲线进行分析。
两种方法均采用具有两个分布室的模型,以及未根据体表面积校正的 CKD-EPI eGFR 方程作为消除率常数(K)的协变量,对数据的描述最佳。参数法的群体参数估计值为 K 0.637 h(个体间变异[BSV]:19.0%变异系数[CV])和中央分布容积(V)29.6 L(无 BSV)。非参数法的值为 K 0.681 h(34.0% CV)和 V 31.1 L(42.6% CV)。
两种模型均能很好地描述亚胺培南的 popPK;参数估计值相似,包含的协变量相同。然而,非参数模型中的估计 BSV 更高。这可能会对给药模拟期间的估计暴露量产生影响,应在模拟研究中进一步探讨。