Department of Clinical and Experimental Epilepsy, University College London, London, UK; Chalfont Centre for Epilepsy and National Hospital for Neurology and Neurosurgery, Queen Square, London, UK.
School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom.
Neuroimage Clin. 2020;25:102174. doi: 10.1016/j.nicl.2020.102174. Epub 2020 Jan 13.
Anterior two-thirds corpus callosotomy is an effective palliative neurosurgical procedure for drug-refractory epilepsy that is most commonly used to treat drop-attacks. Laser interstitial thermal therapy is a novel stereotactic ablative technique that has been utilised as a minimally invasive alternative to resective and disconnective open neurosurgery. Case series have reported success in performing laser anterior two-thirds corpus callosotomy. Computer-assisted planning algorithms may help to automate and optimise multi-trajectory planning for this procedure.
To undertake a simulation-based feasibility study of computer-assisted corpus callostomy planning in comparison with expert manual plans in the same patients.
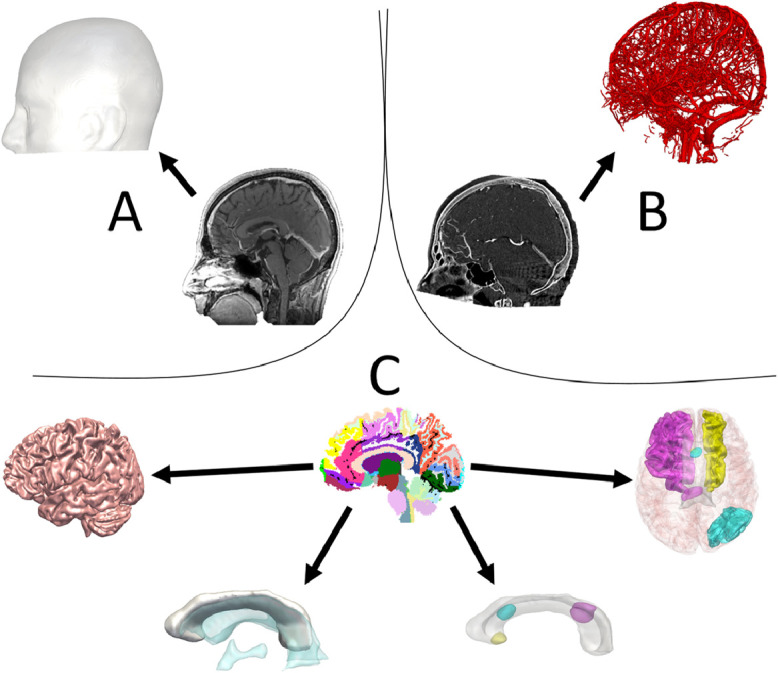
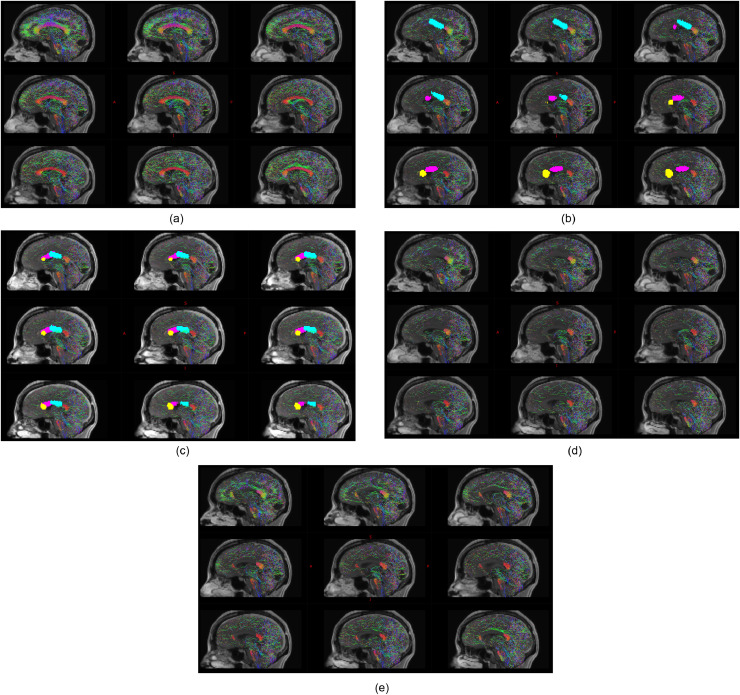
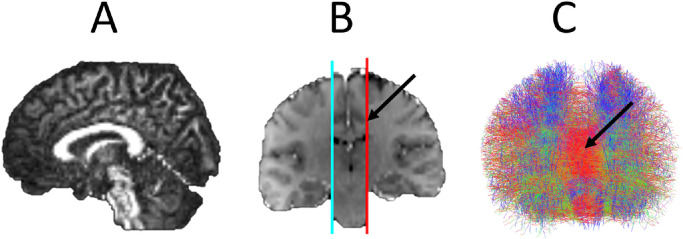
Ten patients were selected from a prospectively maintained database. Patients had previously undergone diffusion-weighted imaging and digital subtraction angiography as part of routine SEEG care. Computer-assisted planning was performed using the EpiNav™ platform and compared to manually planned trajectories from two independent blinded experts. Estimated ablation cavities were used in conjunction with probabilistic tractography to simulate the expected extent of interhemispheric disconnection.
Computer-assisted planning resulted in significantly improved trajectory safety metrics (risk score and minimum distance to vasculature) compared to blinded external expert manual plans. Probabilistic tractography revealed residual interhemispheric connectivity in 1/10 cases following computer-assisted planning compared to 4/10 and 2/10 cases with manual planning.
Computer-assisted planning successfully generates multi-trajectory plans capable of LITT anterior two-thirds corpus callosotomy. Computer-assisted planning may provide a means of standardising trajectory planning and serves as a potential new tool for optimising trajectories. A prospective validation study is now required to determine if this translates into improved patient outcomes.
前部三分之二胼胝体切开术是一种有效的姑息性神经外科手术,用于治疗药物难治性癫痫,最常用于治疗猝倒发作。激光间质热疗是一种新的立体定向消融技术,已被用作替代切除和分离的微创手术。病例系列报告成功地进行了激光前部三分之二胼胝体切开术。计算机辅助规划算法可能有助于自动化和优化该手术的多轨迹规划。
在相同患者中进行基于模拟的计算机辅助胼胝体切开术规划与专家手动计划的可行性研究。
从前瞻性维护的数据库中选择了 10 名患者。这些患者先前已经进行了弥散加权成像和数字减影血管造影术,作为常规 SEEG 护理的一部分。使用 EpiNav™平台进行计算机辅助规划,并与两位独立的盲法专家手动规划的轨迹进行比较。使用估计的消融腔结合概率追踪来模拟预期的半球间断开程度。
与盲法外部专家手动计划相比,计算机辅助规划导致轨迹安全性指标(风险评分和与血管的最小距离)显著改善。概率追踪显示,在计算机辅助规划后,10 例中有 1 例存在残留的半球间连接,而手动规划分别有 4 例和 2 例。
计算机辅助规划成功生成了可用于 LITT 前部三分之二胼胝体切开术的多轨迹计划。计算机辅助规划可能为轨迹规划标准化提供了一种手段,并可作为优化轨迹的潜在新工具。现在需要进行前瞻性验证研究,以确定这是否转化为改善患者的结果。