Kloosterman Mariëlle, van Stipdonk Antonius M W, Ter Horst Iris, Rienstra Michiel, Van Gelder Isabelle C, Vos Marc A, Prinzen Frits W, Meine Matthias, Vernooy Kevin, Maass Alexander H
Department of Cardiology, University of Groningen, University Medical Centre Groningen, PO Box 30.001, Groningen, 9700, RB, The Netherlands.
Department of Cardiology, Maastricht University Medical Center, Maastricht, the Netherlands.
ESC Heart Fail. 2020 Apr;7(2):645-653. doi: 10.1002/ehf2.12624. Epub 2020 Jan 28.
Echocardiographic response after cardiac resynchronization therapy (CRT) is often lesser in ischaemic cardiomyopathy (ICM) than non-ischaemic dilated cardiomyopathy (NIDCM) patients. We assessed the association of heart failure aetiology on the amount of reverse remodelling and outcome of CRT.
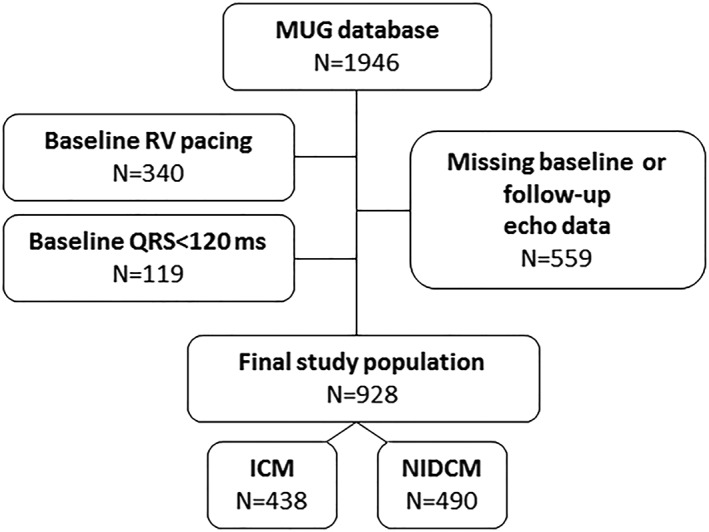
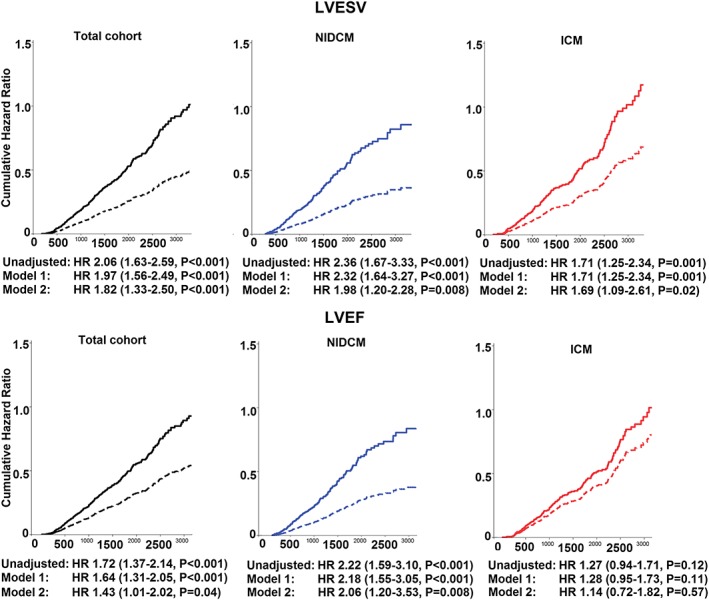
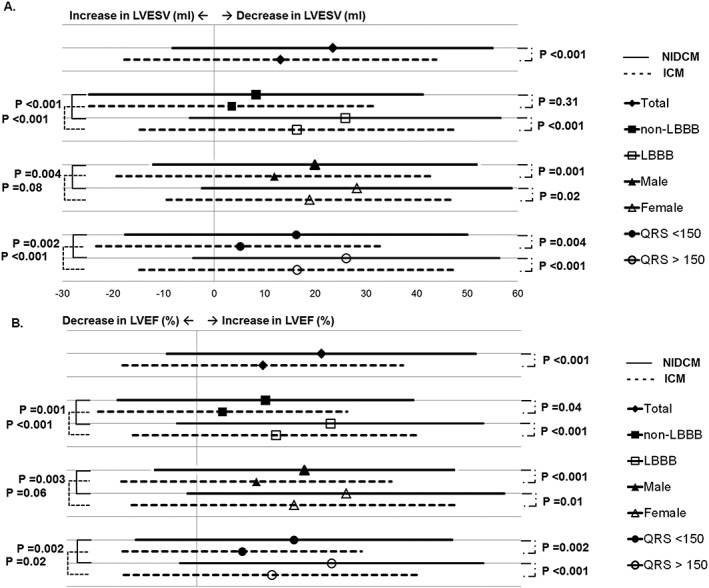
Nine hundred twenty-eight CRT patients were retrospectively included. Reverse remodelling and endpoint occurrence (all-cause mortality, heart transplantation, or left ventricular assist device implantation) was assessed. Two response definitions [≥15% reduction left ventricular end systolic volume (LVESV) and ≥5% improvement left ventricular ejection fraction] and the most accurate cut-off for the amount of reverse remodelling that predicted endpoint freedom were assessed. Mean follow-up was 3.8 ± 2.4 years. ICM was present in 47%. ICM patients who were older (69 ± 7 vs. 63 ± 11), more often men (83% vs. 58%), exhibited less LVESV reduction (13 ± 31% vs. 23 ± 32%) and less left ventricular ejection fraction improvement (5 ± 11% vs. 10 ± 12%) than NIDCM patients (all P < 0.001). Nevertheless, every 1% LVESV reduction was associated with a relative reduction in endpoint occurrence: NIDCM 1.3%, ICM 0.9%, and absolute risk reduction was similar (0.4%). The most accurate cut-off of LVESV reduction that predicted endpoint freedom was 17.1% in NIDCM and 13.2% in ICM.
ICM patients achieve less reverse remodelling than NIDCM, but the prognostic gain in terms of survival time is the same for every single percentage of reverse remodelling that does occur. The assessment and expected magnitude of reverse remodelling should take this effect of heart failure aetiology into account.
心脏再同步治疗(CRT)后,缺血性心肌病(ICM)患者的超声心动图反应通常比非缺血性扩张型心肌病(NIDCM)患者小。我们评估了心力衰竭病因与逆向重构程度及CRT结局之间的关联。
回顾性纳入928例CRT患者。评估逆向重构和终点事件的发生情况(全因死亡率、心脏移植或左心室辅助装置植入)。评估了两种反应定义[左心室收缩末期容积(LVESV)降低≥15%和左心室射血分数提高≥5%]以及预测终点事件未发生的逆向重构程度的最准确截断值。平均随访时间为3.8±2.4年。47%的患者为ICM。与NIDCM患者相比,ICM患者年龄更大(69±7岁对63±11岁),男性比例更高(83%对58%),LVESV降低幅度更小(13±31%对23±32%),左心室射血分数提高幅度更小(5±11%对10±12%)(所有P<0.001)。然而,LVESV每降低1%,终点事件发生的相对风险就会降低:NIDCM为1.3%,ICM为0.9%,绝对风险降低相似(0.4%)。预测终点事件未发生的LVESV降低的最准确截断值在NIDCM中为17.1%,在ICM中为13.2%。
ICM患者的逆向重构程度低于NIDCM,但就生存时间而言,每发生1%的逆向重构,其预后获益是相同的。在评估逆向重构及其预期程度时,应考虑心力衰竭病因的这种影响。