Department of Community Emergency Health and Paramedic Practice, Monash University, Melbourne, Australia.
Ambulance Victoria, Doncaster, Australia.
BMC Emerg Med. 2020 Jan 28;20(1):5. doi: 10.1186/s12873-020-0303-9.
Rapid sequence intubation (RSI) is used to secure the airway of stroke patients. Randomized controlled trial evidence exists to support the use of paramedic RSI for traumatic brain injury (TBI), but cannot necessarily be applied to stroke RSI because of differences between the stroke and TBI patient. To understand if the TBI evidence can be used for stroke RSI, we analysed a retrospective cohort of TBI and strokes to compare how survival is impacted differently by RSI when comparing strokes and TBI.
This study was a retrospective analysis of 10 years of in-hospital and out-of-hospital data for all stroke and TBI patients attended by Ambulance Victoria, Australia. Logistic regression predicted the survival for ischemic and haemorrhagic strokes as well as TBI. The constituents of RSI, such a medications, intubation success and time intervals were analysed against survival using interactions to asses if RSI impacts survival differently for strokes compared to TBI.
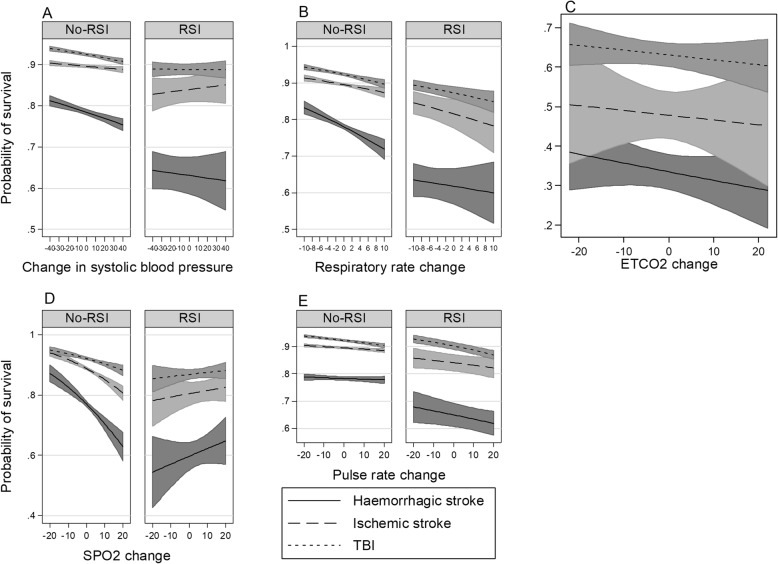
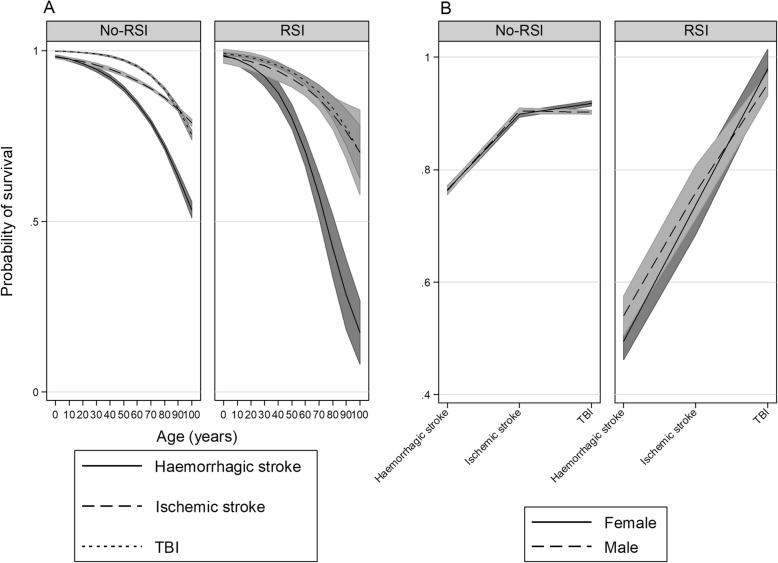
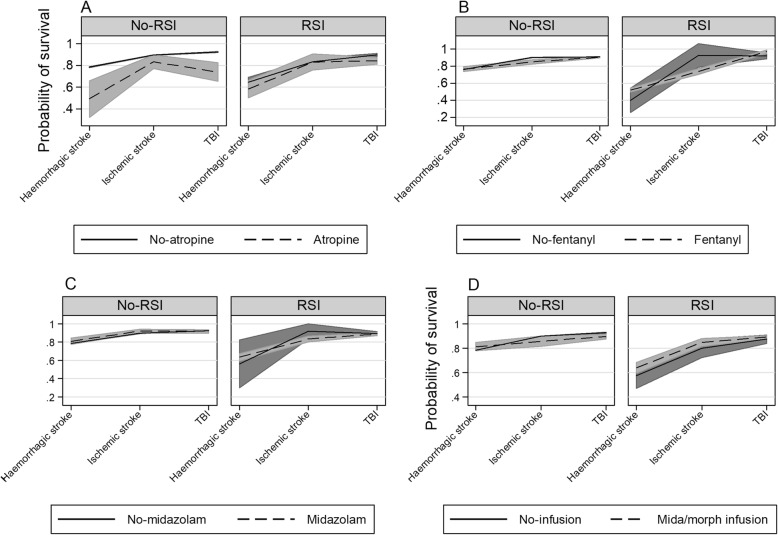
This analysis found significant interactions in the RSI-only group for age, number of intubation attempts, atropine, fentanyl, pulse rate and perhaps scene time and time- to-RSI. Such interactions imply that RSI impact survival differently for TBI versus strokes. Additionally, no significant difference in survival for TBI was found, with a - 0.7% lesser survival for RSI compared to no-RSI; OR 0.86 (95% CI 0.67 to 1.11; p = 0.25). Survival for haemorrhagic stroke was - 14.1% less for RSI versus no-RSI; OR 0.44 (95% CI 0.33 to 0.58; p = 0.01) and was - 4.3%; OR 0.67 (95% CI 0.49 to 0.91; p = 0.01) lesser for ischemic strokes.
Rapid sequence intubation and related factors interact with stroke and TBI, which suggests that RSI effects stroke survival in a different way from TBI. If RSI impact survival differently for strokes compared to TBI, then perhaps the TBI evidence cannot be used for stroke RSI.
快速序贯插管(RSI)用于保障中风患者的气道安全。随机对照试验证据支持使用急救人员进行创伤性脑损伤(TBI)的 RSI,但由于中风和 TBI 患者之间存在差异,该证据不一定适用于中风的 RSI。为了了解 TBI 证据是否可用于中风的 RSI,我们分析了 TBI 和中风的回顾性队列,以比较比较中风和 TBI 时 RSI 对生存率的影响有何不同。
本研究是对澳大利亚维多利亚救护车服务机构 10 年来所有中风和 TBI 患者的住院和院外数据进行的回顾性分析。使用逻辑回归预测缺血性和出血性中风以及 TBI 的生存率。使用交互作用分析 RSI 的组成部分,如药物、插管成功率和时间间隔与生存率的关系,以评估 RSI 对中风的生存影响是否与 TBI 不同。
该分析发现 RSI 组中存在年龄、插管尝试次数、阿托品、芬太尼、脉搏率以及可能的现场时间和到 RSI 的时间的显著交互作用。这些交互作用表明,RSI 对 TBI 和中风的生存影响不同。此外,未发现 TBI 患者的生存率有显著差异,与无 RSI 相比,RSI 使生存率降低了-7%;OR 0.86(95%CI 0.67 至 1.11;p=0.25)。与无 RSI 相比,出血性中风的 RSI 使生存率降低了-14.1%;OR 0.44(95%CI 0.33 至 0.58;p=0.01),而缺血性中风的 RSI 使生存率降低了-4.3%;OR 0.67(95%CI 0.49 至 0.91;p=0.01)。
快速序贯插管和相关因素与中风和 TBI 相互作用,这表明 RSI 对中风的生存影响与 TBI 不同。如果 RSI 对中风的生存影响与 TBI 不同,那么 TBI 的证据可能不能用于中风的 RSI。