Wald Ori, Islam Idais, Amit Korach, Ehud Rudis, Eldad Erez, Omer Or, Aviad Zik, Moshe Shapira Oz, Uzi Izhar
Department of Cardiothoracic Surgery, Hadassah Hebrew University Hospital, Jerusalem, Israel.
Department of Orthopedics, Hadassah Hebrew University Hospital, Jerusalem, Israel.
J Cardiothorac Surg. 2020 Jan 28;15(1):29. doi: 10.1186/s13019-020-1064-y.
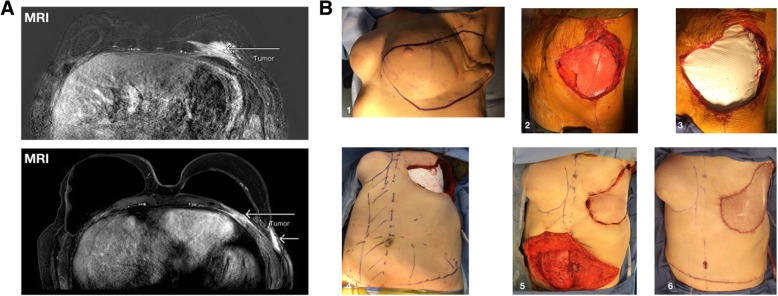
BACKGROUND & OBJECTIVES: Primary chest wall sarcomas are rare and therapeutically challenging tumors. Herein we report the outcomes of a surgery-based multimodality therapy for these pathologies over an 11-year period. In addition, we present a case that illustrates the surgical challenges that extensive chest wall resection may pose.
Using the Society of Thoracic Surgeons general thoracic surgery database, we have prospectively collected data in our institute on all patients undergoing chest wall resection and reconstruction for primary chest wall sarcomas between June 2008-October 2019.
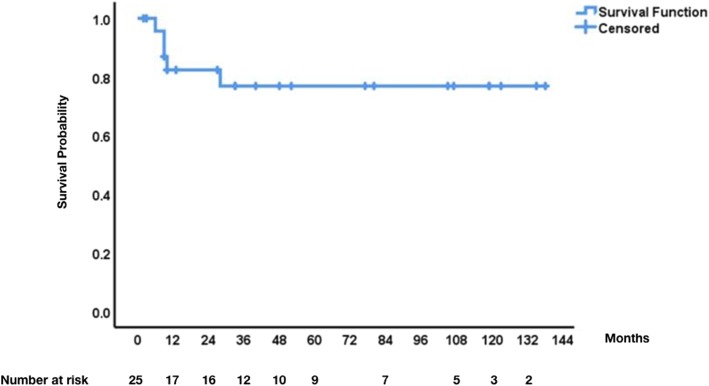
We performed 28 surgical procedures on 25 patients aged 5 to 91 years (median age 33). Eleven tumors were bone- and cartilage-derived and 14 tumors originated from soft tissue elements. Seven patients (7/25, 28%) received neo-adjuvant therapy and 14 patients (14/25, 56%) received adjuvant therapy. The median number of ribs that were resected was 2.5 (range 0 to 6). In 18/28 (64%) of surgeries, additional skeletal or visceral organs were removed, including: diaphragm [1], scapula [2], sternum [2], lung [2], vertebra [1], clavicle [1] and colon [1]. Chest wall reconstruction was deemed necessary in 16/28 (57%) of cases, polytetrafluoroethylene (PTFE) Gore-Tex patches was used in 13/28 (46%) of cases and biological flaps where used in 4/28 (14%) of cases. R0, R1 and R2 resection margins were achieved in 19/28 (68%), 9/28 (32%) and 0/28 (0%) of cases, respectively. The median follow up time was 33 months (range 2 to 138). During the study period, disease recurred in 8/25 (32%) of patients. Of these, 3 were re-operated on and are free of disease. At date of last follow up, 5/25 (20%) of patients have died due to their disease and in contrast, 20/25 (80%) were alive with no evidence of disease.
Surgery-based multimodality therapy is an effective treatment approach for primary chest wall sarcomas. Resection of additional skeletal or visceral organs and reconstruction with synthetic and/or biological flaps is often required in order to obtain R0 resection margins. Ultimately, long-term survival in this clinical scenario is an achievable goal.
原发性胸壁肉瘤是一种罕见且治疗具有挑战性的肿瘤。在此,我们报告了11年间针对这些病症采用以手术为主的多模式治疗的结果。此外,我们还展示了一个病例,该病例说明了广泛胸壁切除可能带来的手术挑战。
利用胸外科医师协会普通胸外科数据库,我们前瞻性地收集了我院2008年6月至2019年10月期间所有因原发性胸壁肉瘤接受胸壁切除及重建手术患者的数据。
我们对25例年龄在5至91岁(中位年龄33岁)的患者进行了28例手术。11例肿瘤起源于骨和软骨,14例肿瘤起源于软组织成分。7例患者(7/25,28%)接受了新辅助治疗,14例患者(14/25,56%)接受了辅助治疗。切除肋骨的中位数为2.5根(范围为0至6根)。在18/28(64%)的手术中,还切除了其他骨骼或内脏器官,包括:膈肌[1例]、肩胛骨[2例]、胸骨[2例]、肺[2例]、椎体[1例]、锁骨[1例]和结肠[1例]。16/28(57%)的病例认为有必要进行胸壁重建,13/28(46%)的病例使用了聚四氟乙烯(PTFE)戈尔特斯补片,4/28(14%)的病例使用了生物瓣。R0、R1和R2切除切缘分别在19/28(68%)、9/28(32%)和0/28(0%)的病例中实现。中位随访时间为33个月(范围为2至138个月)。在研究期间,8/25(32%)的患者疾病复发。其中,3例再次接受手术,目前无疾病。在最后一次随访时,5/25(20%)的患者因疾病死亡,相比之下,20/25(80%)的患者存活且无疾病证据。
以手术为主的多模式治疗是原发性胸壁肉瘤的有效治疗方法。为了获得R0切除切缘,通常需要切除其他骨骼或内脏器官,并使用合成和/或生物瓣进行重建。最终,在这种临床情况下实现长期生存是一个可以实现的目标。