Department of Surgery, East Carolina University, Greenville, North Carolina;
Department of Surgery and.
Clin J Am Soc Nephrol. 2020 Feb 7;15(2):228-237. doi: 10.2215/CJN.06660619. Epub 2020 Jan 28.
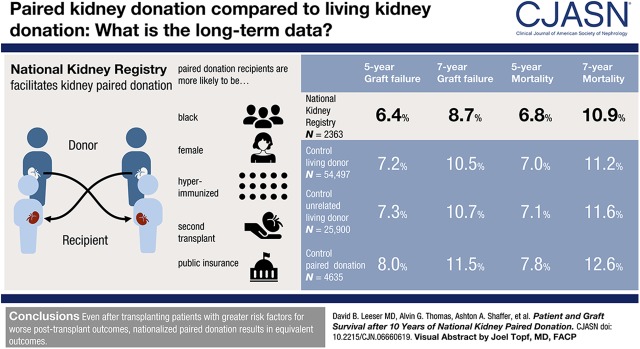
In the United States, kidney paired donation networks have facilitated an increasing proportion of kidney transplants annually, but transplant outcome differences beyond 5 years between paired donation and other living donor kidney transplant recipients have not been well described.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Using registry-linked data, we compared National Kidney Registry (=2363) recipients to control kidney transplant recipients (=54,497) (February 2008 to December 2017). We estimated the risk of death-censored graft failure and mortality using inverse probability of treatment weighted Cox regression. The parsimonious model adjusted for recipient factors (age, sex, black, race, body mass index ≥30 kg/m, diabetes, previous transplant, preemptive transplant, public insurance, hepatitis C, eGFR, antibody depleting induction therapy, year of transplant), donor factors (age, sex, Hispanic ethnicity, body mass index ≥30 kg/m), and transplant factors (zero HLA mismatch).
National Kidney Registry recipients were more likely to be women, black, older, on public insurance, have panel reactive antibodies >80%, spend longer on dialysis, and be previous transplant recipients. National Kidney Registry recipients were followed for a median 3.7 years (interquartile range, 2.1-5.6; maximum 10.9 years). National Kidney Registry recipients had similar graft failure (5% versus 6%; log-rank =0.2) and mortality (9% versus 10%; log-rank =0.4) incidence compared with controls during follow-up. After adjustment for donor, recipient, and transplant factors, there no detectable difference in graft failure (adjusted hazard ratio, 0.95; 95% confidence interval, 0.77 to 1.18; =0.6) or mortality (adjusted hazard ratio, 0.86; 95% confidence interval, 0.70 to 1.07; =0.2) between National Kidney Registry and control recipients.
Even after transplanting patients with greater risk factors for worse post-transplant outcomes, nationalized paired donation results in equivalent outcomes when compared with control living donor kidney transplant recipients.
在美国,肾脏配对捐赠网络每年促成的肾脏移植比例不断增加,但配对捐赠与其他活体供肾移植受者 5 年以上的移植结局差异尚未得到充分描述。
设计、地点、参与者和测量:利用注册相关数据,我们将国家肾脏登记处(=2363 名)受者与对照组(=54497 名)(2008 年 2 月至 2017 年 12 月)进行比较。我们使用逆概率治疗加权 Cox 回归来估计死亡风险校正移植物失败和死亡率。简约模型调整了受者因素(年龄、性别、黑人、种族、体质指数≥30kg/m2、糖尿病、既往移植、优先移植、公共保险、丙型肝炎、eGFR、抗体耗竭诱导治疗、移植年份)、供者因素(年龄、性别、西班牙裔、体质指数≥30kg/m2)和移植因素(零 HLA 错配)。
国家肾脏登记处的受者更可能是女性、黑人、年龄较大、接受公共保险、具有>80%的反应性抗体、透析时间更长且为既往移植受者。国家肾脏登记处的受者中位随访时间为 3.7 年(四分位距,2.1-5.6;最长 10.9 年)。在随访期间,与对照组相比,国家肾脏登记处的受者发生移植物失败(5%对 6%;对数秩=0.2)和死亡率(9%对 10%;对数秩=0.4)相似。在调整供者、受者和移植因素后,国家肾脏登记处与对照组受者之间的移植物失败(调整后的危险比,0.95;95%置信区间,0.77 至 1.18;=0.6)或死亡率(调整后的危险比,0.86;95%置信区间,0.70 至 1.07;=0.2)均无显著差异。
即使将具有更差移植后结局风险因素的患者进行移植,国家化的配对捐赠与对照组活体供肾移植受者的结果相当。