Al Harbi Mohammed K, Alattas Khaled A, Alnajar Muhanad, Albuthi Muneera F
Department of Anesthesia, King Abdulaziz Medical City, Riyadh, Saudi Arabia.
Saudi J Anaesth. 2020 Jan-Mar;14(1):123-126. doi: 10.4103/sja.SJA_165_19. Epub 2020 Jan 6.
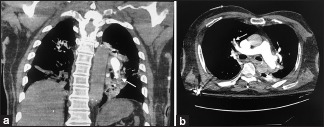
An 80-year-old male patient presented with 2 weeks history of low back pain undergoing posterior spinal fusion with laminectomy in the prone position. The patient was induced with fentanyl, propofol, and rocuronium, and then he was positioned in the prone position. After 6 h of starting the surgery, the patient started to be hypotension and bradycardia followed by pulseless electrical activity (PEA). Code blue was activated intraoperatively with immediate initiation of cardiopulmonary resuscitation (CPR) in the prone position and multiple epinephrine boluses. Fortunately, the patient had return of spontaneous circulation. After stabilization, he was taken for computed tomography scan which showed massive pulmonary embolization and management was continued in the intensive care unit. CPR in the prone position has shown to be effective for return of spontaneous circulation after PEA.
一名80岁男性患者,有2周的腰痛病史,在俯卧位下行后路脊柱融合术及椎板切除术。患者用芬太尼、丙泊酚和罗库溴铵诱导麻醉,然后置于俯卧位。手术开始6小时后,患者开始出现低血压和心动过缓,随后出现无脉电活动(PEA)。术中启动蓝色急救代码,立即在俯卧位进行心肺复苏(CPR)并多次推注肾上腺素。幸运的是,患者恢复了自主循环。病情稳定后,他接受了计算机断层扫描,结果显示有大面积肺栓塞,随后在重症监护病房继续治疗。俯卧位心肺复苏已被证明对PEA后恢复自主循环有效。