Bakshi Sabyasachi
Department of General surgery, BSMCH, Bankura, West Bengal, PIN-722102, India.
, Kathghara Lane, Sonatuli, Hooghly, West Bengal, PIN-712103, India.
BMC Surg. 2020 Jan 30;20(1):20. doi: 10.1186/s12893-020-0688-0.
Pancreatic pseudocyst is a very common benign cystic lesion of the pancreas. It develops in 5-15% of patients with peri-pancreatic fluid collection following acute pancreatitis. Collection usually occurs within the lesser sac of the omentum (near the pancreatic head and body region). But in 20-22% cases, that may be extra-pancreatic like in the mediastinum, pleura, in the peritoneal cavity including the pelvis. The pancreatic pseudocyst typically contains brownish fluid with necrotic tissue sludge which may get infected giving rise to infected pseudocyst or pancreatic abscess. The present case is an unusual condition of a young alcoholic subject who was finally diagnosed as a case of a pancreatic abscess within hepato-gastric ligament and was managed with operative intervention. To the best of the author's knowledge, it is the first-ever reported case of a pancreatic abscess within the hepato-gastric ligament in the world. Literature was reviewed to explore potential etiopathogenesis and therapeutic strategies of this extremely rare condition.
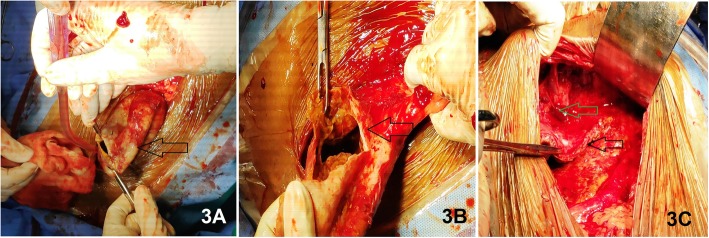
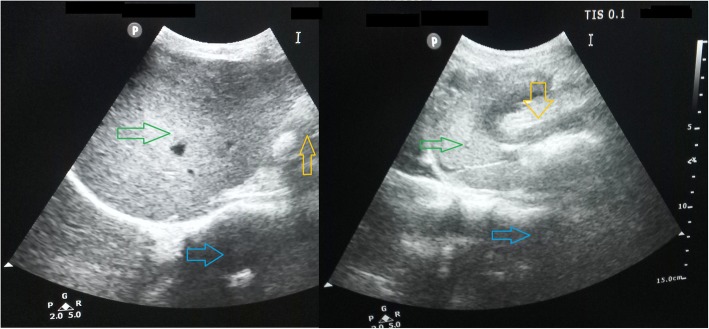
A 38 years old gentleman, chronic alcoholic, having a previous history of acute pancreatitis 3 months back, presented with fever (102 degrees Fahrenheit) and a huge [20 cm (horizontal) X 15 cm (vertical)] severely painful swelling in the epigastric region. The swelling was round-shaped, intra-abdominal, fixed to deeper tissue, tense-cystic, poorly trans-illuminant, non-pulsatile and irreducible. Routine blood tests showed leucocytosis (14,500/mm) with neutrophilia and elevated plasma pancreatic amylase and lipase levels. USG and MDCT scan of the whole abdomen revealed a thick-walled echogenic cystic swelling of size 18 cm × 12 cm in the epigastric region. USG guided aspiration of the cyst revealed mixed purulent brownish fluid. The cyst fluid was negative for mucin stain and contained high amylase level with low CEA level, suggesting infected pancreatic pseudocyst. An open drainage procedure was considered through an upper midline laparotomy. Aspiration of the pus mixed cyst fluid along with tissue debris was done. Through irrigation of the cyst was done with normal saline. The cyst wall was de-roofed leaving a small part adherent to the inferior surface of the left lobe of the liver. Later the cyst fluid culture showed significant growth of Escherichia coli. He was put on IV antibiotics. The patient was discharged in a stable condition after 5 days. The histopathological examination confirmed pancreatic abscess. Six months after the operation, the patient is doing well, remaining asymptomatic and there is no sign of recurrence.
Due to extreme rarity, pancreatic abscess formation within hepato-gastric ligament may be a diagnostic dilemma and requires a high index of suspicion. Surgeons should be aware of this rare clinical entity for prompt management of potential morbidity.
胰腺假性囊肿是胰腺非常常见的良性囊性病变。在急性胰腺炎后胰周积液的患者中,其发生率为5% - 15%。积液通常发生在网膜囊内(胰头和胰体区域附近)。但在20% - 22%的病例中,可能位于胰腺外,如纵隔、胸膜、包括盆腔在内的腹腔。胰腺假性囊肿通常含有带坏死组织残渣的褐色液体,可能会发生感染,导致感染性假性囊肿或胰腺脓肿。本病例是一名年轻酗酒者的特殊情况,最终被诊断为肝胃韧带内胰腺脓肿,并接受了手术干预。据作者所知,这是世界上首例报道的肝胃韧带内胰腺脓肿病例。回顾文献以探讨这种极其罕见情况的潜在病因和治疗策略。
一名38岁男性,慢性酗酒者,3个月前有急性胰腺炎病史,现出现发热(华氏102度),上腹部有一个巨大的[20厘米(横径)×15厘米(纵径)]剧痛性肿胀。肿胀呈圆形,位于腹腔内,与深部组织固定,紧张呈囊性,透光性差,无搏动且不可回纳。常规血液检查显示白细胞增多(14,500/mm)伴中性粒细胞增多,血浆胰淀粉酶和脂肪酶水平升高。全腹部超声和多层螺旋CT扫描显示上腹部有一个大小为18厘米×12厘米的厚壁高回声囊性肿胀。超声引导下囊肿穿刺抽出混合脓性褐色液体。囊肿液粘蛋白染色阴性,淀粉酶水平高而癌胚抗原水平低,提示感染性胰腺假性囊肿。考虑通过上腹部正中剖腹术进行开放引流。抽出脓性混合囊肿液及组织碎片,并用生理盐水冲洗囊肿。囊肿去顶,使一小部分与肝左叶下表面粘连。随后囊肿液培养显示大肠杆菌大量生长。给予静脉抗生素治疗。患者5天后病情稳定出院。组织病理学检查证实为胰腺脓肿。术后6个月,患者情况良好,无症状,无复发迹象。
由于极其罕见,肝胃韧带内胰腺脓肿可能是一个诊断难题,需要高度怀疑。外科医生应了解这种罕见的临床实体,以便及时处理潜在的发病率。