Department of Radiation Oncology, Advanced Centre for Treatment Research and Education in Cancer, Tata Memorial Centre, Homi Bhabha National Institute, Kharghar, Navi Mumbai, Maharashtra, India.
Department of Radiation Oncology and Medical Physics, Tata Memorial Hospital, Tata Memorial Centre, Homi Bhabha National Institute, Parel, Mumbai, Maharashtra, India.
Radiat Oncol. 2020 Jan 30;15(1):22. doi: 10.1186/s13014-020-1473-z.
To ascertain the dosimetric performance of a new delivery system (the Halcyon system, H) equipped with dual-layer stacked multi-leaf collimator (MLC) for risk-adapted targets in cervix uteri cancer patients compared to another ring-based system in clinical operation (Helical Tomotherapy, HT).
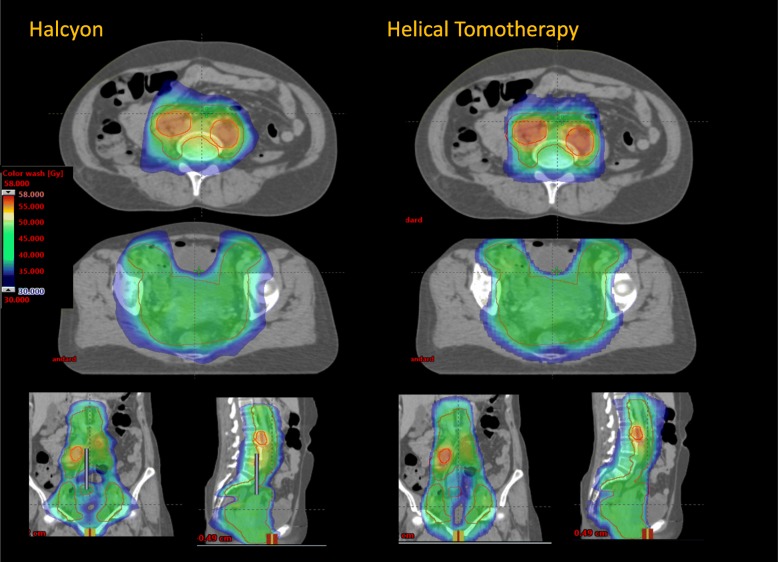
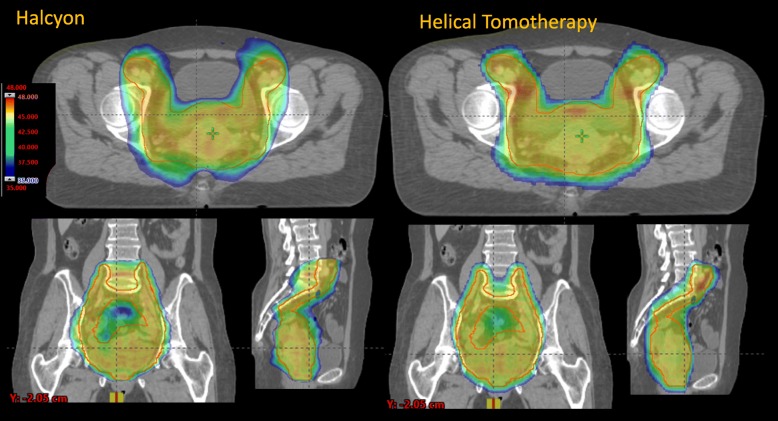
Twenty patients were retrospectively included in a treatment planning study (10 with positive lymph nodes and 10 without). The dose prescription (45Gy to the primary tumour volume and a simultaneously integrated boost up to 55Gy for the positive patients) and the clinical planning objectives were defined consistently as recommended by an ongoing multicentric clinical trial. Halcyon plans were optimised for the volumetric modulated arc therapy. The plan comparison was performed employing the quantitative analysis of the dose-volume histograms.
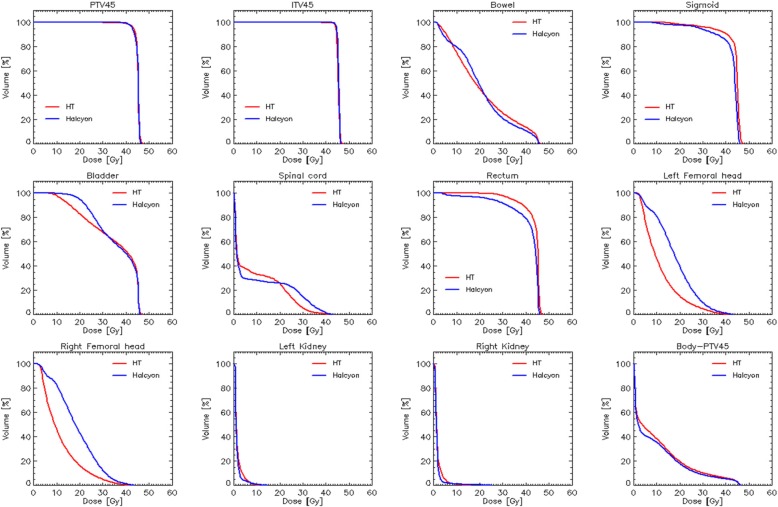
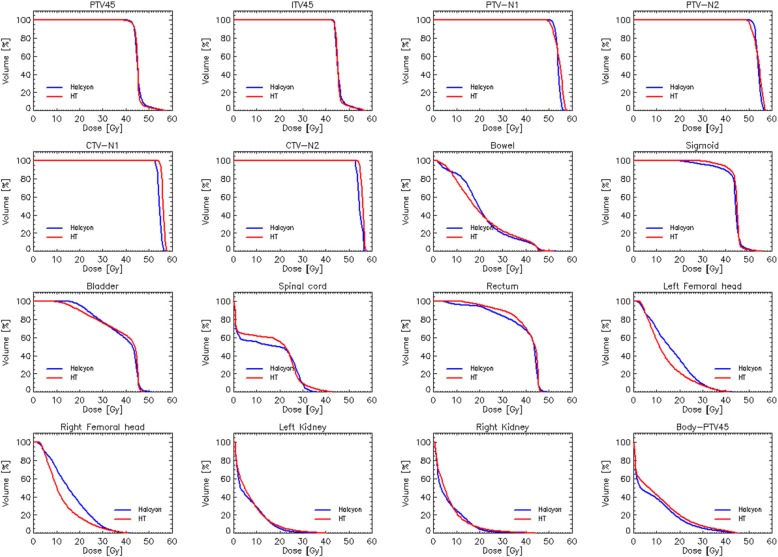
The coverage of the primary and nodal target volumes was comparable for both techniques and both subsets of patients. The primary planning target volume (PTV) receiving at least 95% of the prescription isodose ranged from 97.2 ± 1.1% (node-negative) to 99.1 ± 1.2% (node-positive) for H and from 96.5 ± 1.9% (node-negative) to 98.3 ± 0.9% (node-positive) for HT. The uncertainty is expressed at one standard deviation from the cohort of patient per each group. For the nodal clinical target volumes, the dose received by 98% of the planning target volume ranged 55.5 ± 0.1 to 56.0 ± 0.8Gy for H and HT, respectively. The only significant and potentially relevant differences were observed for the bowels. In this case, V resulted 226.3 ± 35.9 and 186.9 ± 115.9 cm for the node-positive and node-negative patients respectively for Halcyon. The corresponding findings for HT were: 258.9 ± 60.5 and 224.9 ± 102.2 cm. On the contrary, V resulted 1279.7 ± 296.5 and 1557.2 ± 359.9 cm for HT and H respectively for node-positive and 1010.8 ± 320.9 versus 1203.8 ± 332.8 cm for node-negative.
This retrospective treatment planning study, based on the dose constraints derived from the Embrace II study protocol, suggested the essential equivalence between Halcyon based and Helical Tomotherapy based plans for the intensity-modulated rotational treatment of cervix uteri cancer. Different levels of sparing were observed for the bowels with H better protecting in the high-dose region and HT in the mid-low dose regions. The clinical impact of these differences should be further addressed.
比较配备双层堆叠多叶准直器(MLC)的新型输送系统( Halcyon 系统,H)与临床应用中的另一种基于环形的系统(螺旋断层放疗,HT)在宫颈癌风险适应靶区的剂量学性能。
回顾性纳入 20 例患者进行治疗计划研究(10 例淋巴结阳性,10 例淋巴结阴性)。剂量处方(原发肿瘤体积 45Gy,阳性患者同时进行一体化增敏 55Gy)和临床计划目标与正在进行的多中心临床试验一致。 Halcyon 计划采用容积调强弧形治疗进行优化。通过剂量体积直方图的定量分析进行计划比较。
两种技术和两种患者亚组的主要和淋巴结靶区覆盖范围相当。接受至少 95%处方等剂量线的原发计划靶区(PTV)范围为 H 组 97.2±1.1%(淋巴结阴性)至 99.1±1.2%(淋巴结阳性),HT 组 96.5±1.9%(淋巴结阴性)至 98.3±0.9%(淋巴结阳性)。每个组的每个患者的不确定性均表示为一个标准差。对于淋巴结临床靶区,计划靶区体积的 98%接受的剂量范围分别为 H 组 55.5±0.1 至 56.0±0.8Gy 和 HT 组。仅观察到有潜在相关意义的显著差异与肠道有关。在这种情况下, Halcyon 组的淋巴结阳性和淋巴结阴性患者的 V 结果分别为 226.3±35.9 和 186.9±115.9cm。HT 的相应结果为:258.9±60.5 和 224.9±102.2cm。相反,HT 组的 V 结果分别为 1010.8±320.9 和 1203.8±332.8cm,而 H 组的 V 结果分别为 1557.2±359.9 和 1279.7±296.5cm。
这项基于 Embrace II 研究方案得出的剂量限制的回顾性治疗计划研究表明,在宫颈癌的强度调制旋转治疗中,基于 Halcyon 的计划与基于螺旋断层放疗的计划基本等效。对于肠道,H 更好地保护高剂量区域,HT 更好地保护中低剂量区域,观察到不同程度的保护。这些差异的临床影响需要进一步研究。