Moffitt Cancer Center, Tampa, FL, USA.
Ascension Columbia St. Mary's Hospital, Milwaukee, WI, USA.
BMC Cancer. 2020 Jan 31;20(1):81. doi: 10.1186/s12885-020-6534-z.
Increased usage of genomic risk assessment assays suggests increased reliance on data provided by these assays to guide therapy decisions. The current study aimed to assess the change in treatment decision and physician confidence based on the 70-gene risk of recurrence signature (70-GS, MammaPrint) and the 80-gene molecular subtype signature (80-GS, BluePrint) in early stage breast cancer patients.
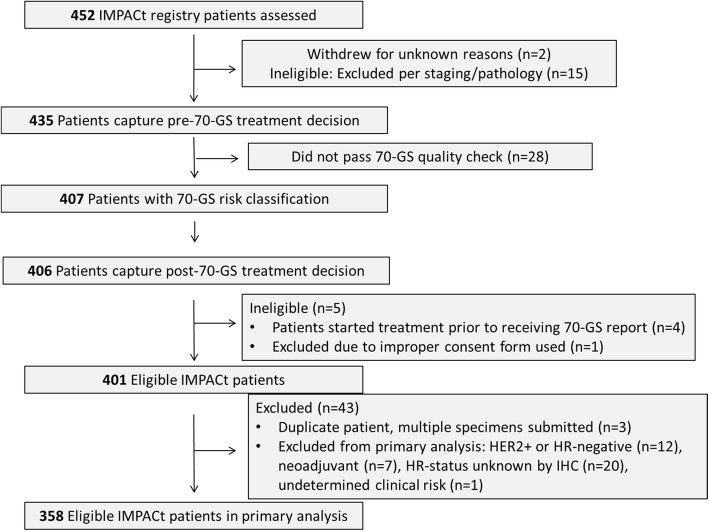
IMPACt, a prospective, case-only study, enrolled 452 patients between November 2015 and August 2017. The primary objective population included 358 patients with stage I-II, hormone receptor-positive, HER2-negative breast cancer. The recommended treatment plan and physician confidence were captured before and after receiving results for 70-GS and 80-GS. Treatment was started after obtaining results. The distribution of 70-GS High Risk (HR) and Low Risk (LR) patients was evaluated, in addition to the distribution of 80-GS compared to IHC status.
The 70-GS classified 62.5% (n = 224/358) of patients as LR and 37.5% (n = 134/358) as HR. Treatment decisions were changed for 24.0% (n = 86/358) of patients after receiving 70-GS and 80-GS results. Of the LR patients initially prescribed CT, 71.0% (44/62) had CT removed from their treatment recommendation. Of the HR patients not initially prescribed CT, 65.1% (41/63) had CT added. After receiving 70-GS results, CT was included in 83.6% (n = 112/134) of 70-GS HR patient treatment plans, and 91.5% (n = 205/224) of 70-GS LR patient treatment plans did not include CT. For patients who disagreed with the treatment recommended by their physicians, most (94.1%, n = 16/17) elected not to receive CT when it was recommended. For patients whose physician-recommended treatment plan was discordant with 70-GS results, discordance was significantly associated with age and lymph node status.
The IMPACt trial showed that treatment plans were 88.5% (n = 317/358) in agreement with 70-GS results, indicating that physicians make treatment decisions in clinical practice based on the 70-GS result. In clinically high risk, 70-GS Low Risk patients, there was a 60.0% reduction in treatment recommendations that include CT. Additionally, physicians reported having greater confidence in treatment decisions for their patients in 72% (n = 258/358) of cases after receiving 70-GS results.
"Measuring the Impact of MammaPrint on Adjuvant and Neoadjuvant Treatment in Breast Cancer Patients: A Prospective Registry" (NCT02670577) retrospectively registered on Jan 27, 2016.
基因组风险评估检测的使用增加表明人们越来越依赖这些检测结果来指导治疗决策。本研究旨在评估 70 基因复发风险签名(70-GS,MammaPrint)和 80 基因分子亚型签名(80-GS,BluePrint)在早期乳腺癌患者中改变治疗决策和医生信心的情况。
IMPACt 是一项前瞻性、仅病例研究,于 2015 年 11 月至 2017 年 8 月期间纳入了 452 例患者。主要目标人群包括 358 例 I 期-II 期、激素受体阳性、HER2 阴性乳腺癌患者。在接受 70-GS 和 80-GS 结果前后,分别记录了推荐的治疗计划和医生信心。在获得结果后开始治疗。评估了 70-GS 高风险(HR)和低风险(LR)患者的分布情况,以及 80-GS 与 IHC 状态的分布情况。
70-GS 将 62.5%(n=224/358)的患者分类为 LR,37.5%(n=134/358)为 HR。70-GS 和 80-GS 结果改变了 24.0%(n=86/358)患者的治疗决策。最初被处方 CT 的 LR 患者中,有 71.0%(n=44/62)的患者将 CT 从治疗建议中去除。在最初未被处方 CT 的 HR 患者中,有 65.1%(n=41/63)的患者添加了 CT。接受 70-GS 结果后,83.6%(n=112/134)的 70-GS HR 患者治疗计划中包含 CT,91.5%(n=205/224)的 70-GS LR 患者治疗计划中不包括 CT。对于不同意医生推荐治疗的患者,大多数(94.1%,n=16/17)在推荐 CT 时选择不接受。对于医生推荐的治疗计划与 70-GS 结果不一致的患者,不一致与年龄和淋巴结状态显著相关。
IMPACt 试验表明,治疗计划与 70-GS 结果一致的比例为 88.5%(n=317/358),表明医生在临床实践中根据 70-GS 结果做出治疗决策。在临床高风险的 70-GS LR 患者中,包含 CT 的治疗建议减少了 60.0%。此外,在接受 70-GS 结果后,72%(n=258/358)的患者报告说,他们对患者的治疗决策更有信心。
“测量 MammaPrint 在乳腺癌患者辅助和新辅助治疗中的影响:一项前瞻性登记”(NCT02670577)于 2016 年 1 月 27 日进行了回顾性注册。