Amsterdam UMC, Heart Center, Department of Clinical and Experimental Cardiology, Amsterdam Cardiovascular Sciences, University of Amsterdam, Meibergdreef 9, Amsterdam, The Netherlands.
Division of Cardiology, Department of Internal Medicine, Faculty of Medicine, Prince of Songkla University, Songkhla, Thailand.
Clin Res Cardiol. 2020 Sep;109(9):1125-1139. doi: 10.1007/s00392-020-01604-1. Epub 2020 Jan 31.
The efficacy of antiplatelet therapies following percutaneous coronary intervention (PCI) may be affected by body mass index (BMI).
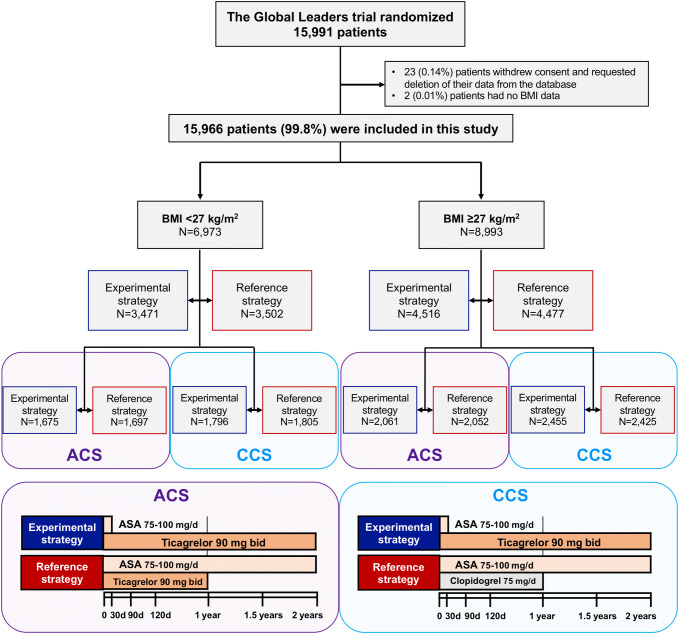
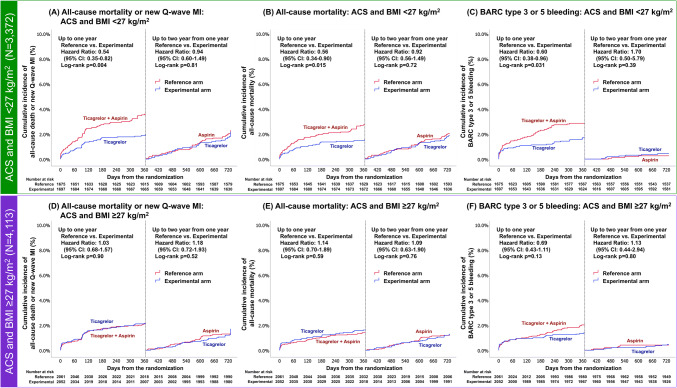
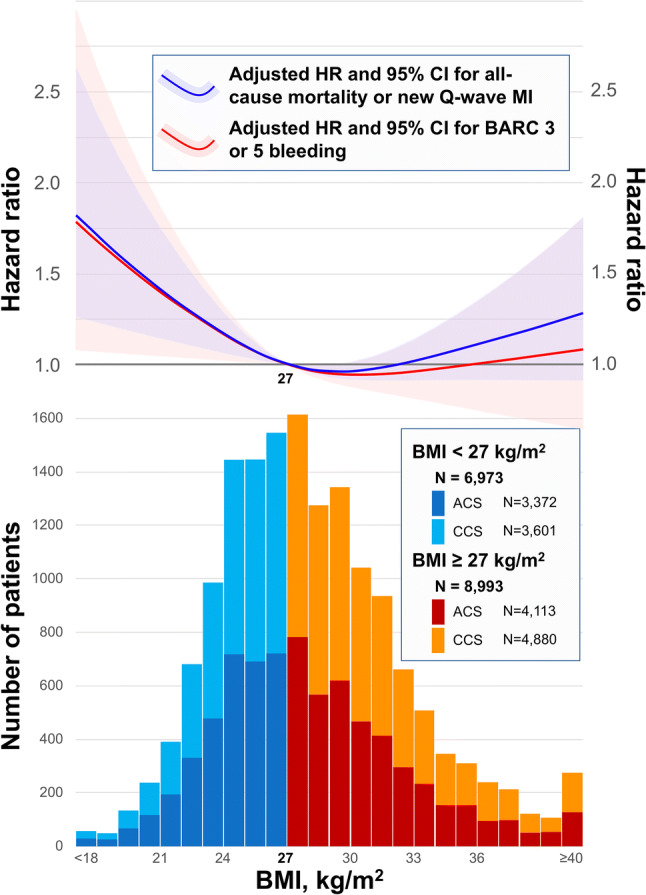
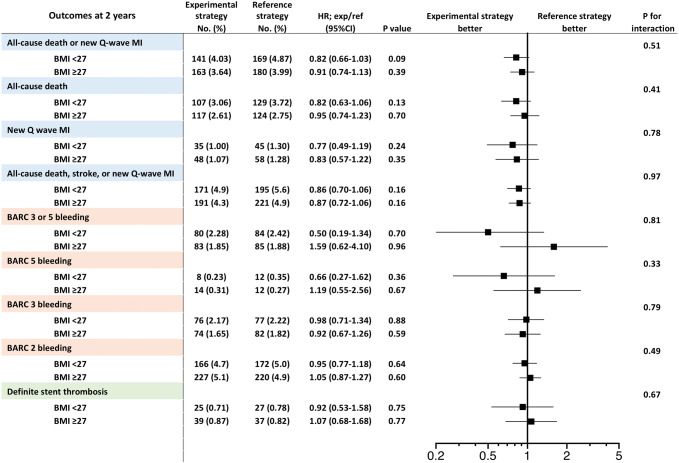
This is a prespecified subgroup analysis of the GLOBAL LEADERS trial, a prospective, multicenter, open-label, randomized controlled trial in an all-comer population undergoing PCI, comparing the experimental strategy (23-month ticagrelor monotherapy following 1-month dual antiplatelet therapy [DAPT]) with a reference regimen (12-month aspirin monotherapy following 12-month DAPT). A total of 15,968 patients were stratified by baseline BMI with prespecified threshold of 27 kg/m. Of those, 6973 (43.7%) patients with a BMI < 27 kg/m had a higher risk of all-cause mortality at 2 years than those with BMI ≥ 27 kg/m (adjusted HR 1.24, 95% CI 1.02-1.49). At 2 years, the rates of the primary endpoint (all-cause mortality or new Q-wave myocardial infarction) were similar between treatment strategies in either BMI group (p = 0.51). In acute coronary syndrome, however, the experimental strategy was associated with significant reduction of the primary endpoint compared to the reference strategy in patients with BMI < 27 kg/m (HR 0.69, 95% CI 0.51-0.94), but not in the ones with BMI ≥ 27 kg/m (p = 0.047). In chronic coronary syndrome, there was no between-group difference in the efficacy and safety of the two antiplatelet strategies.
Overall, BMI did not influence the treatment effect seen with ticagrelor monotherapy; however, a beneficial effect of ticagrelor monotherapy was seen in ACS patients with BMI < 27 kg/m.
The trial has been registered with ClinicalTrials.gov, Number NCT01813435.
经皮冠状动脉介入治疗(PCI)后抗血小板治疗的疗效可能受体重指数(BMI)的影响。
这是 GLOBAL LEADERS 试验的一项预先指定的亚组分析,该试验是一项在所有接受 PCI 的患者中进行的前瞻性、多中心、开放性、随机对照试验,比较了实验策略(1 个月双联抗血小板治疗[DAPT]后 23 个月替格瑞洛单药治疗)与参考方案(12 个月 DAPT 后 12 个月阿司匹林单药治疗)。根据基线 BMI 进行分层,BMI 预设阈值为 27kg/m。其中,6973 名(43.7%)BMI<27kg/m 的患者与 BMI≥27kg/m 的患者相比,2 年时全因死亡率风险更高(校正 HR 1.24,95%CI 1.02-1.49)。在 2 年时,两种 BMI 组中治疗策略的主要终点(全因死亡率或新发 Q 波心肌梗死)发生率相似(p=0.51)。然而,在急性冠状动脉综合征中,与参考策略相比,实验策略在 BMI<27kg/m 的患者中显著降低了主要终点事件的发生率(HR 0.69,95%CI 0.51-0.94),但在 BMI≥27kg/m 的患者中则不然(p=0.047)。在慢性冠状动脉综合征中,两种抗血小板策略的疗效和安全性在组间无差异。
总体而言,BMI 并未影响替格瑞洛单药治疗的疗效;然而,在 BMI<27kg/m 的 ACS 患者中,替格瑞洛单药治疗具有有益效果。
该试验已在 ClinicalTrials.gov 注册,编号为 NCT01813435。