Hamed Jehan M E, Refaat Hesham S M, Al-Wadaani Hamed
Department of Anesthesia and ICU, Faculty of Medicine, Tanta University, Tanta, Egypt.
Department of Surgery, Faculty of Medicine, King Faisal University, Al-Hassa, KSA.
Anesth Essays Res. 2019 Oct-Dec;13(4):636-642. doi: 10.4103/aer.AER_126_19. Epub 2019 Dec 16.
Evaluation of postoperative (PO) analgesic effects of intraoperative (IO) Dexmedetomidine (DEX) compared to remifentanil (REMI) infusions during sevoflurane anesthesia for laparoscopic gastric sleeve surgery.
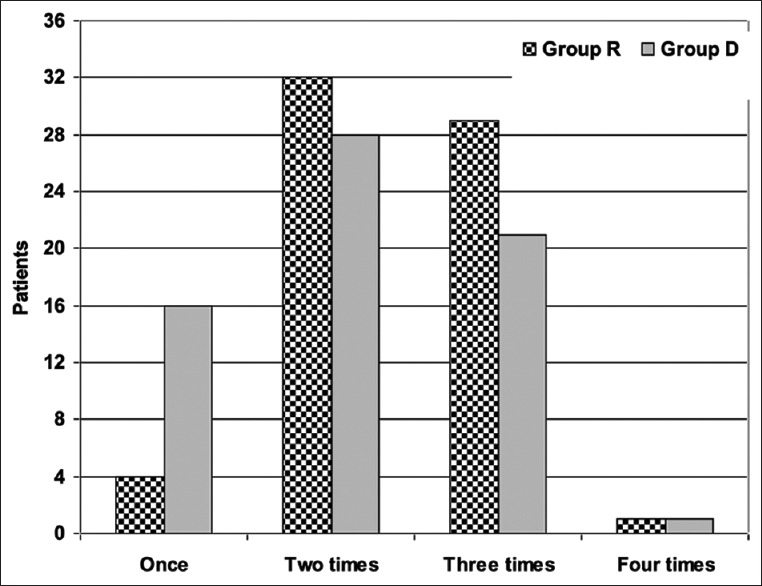
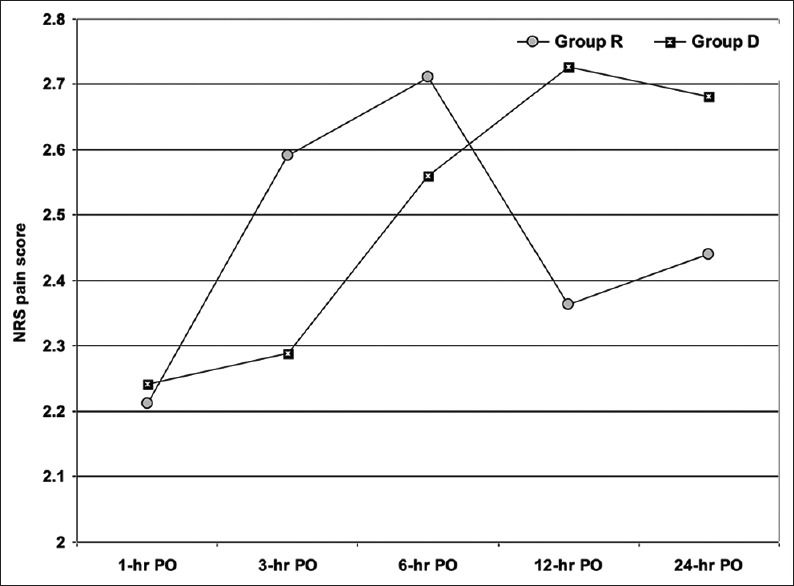
One hundred and thirty-two patients with body mass index >35 kg.m and ASA Grades II or III were randomly divided into group R received REMI infusion (6-18 μg.kg.h) and Group D received DEX infusion (0.2-0.5 μg.kg.h) after tracheal intubation till before stoppage of inhalational anesthetic. Heart rate and mean arterial pressure were noninvasively monitored during and after surgery. Emergence time, time until postanesthetic care unit transfer, and total operating room (OR) time was recorded. PO shoulder-tip pain and wound pain scores were recorded and rescue analgesia was provided as 50 mg pethidine intramuscular injection. Occurrence of PO nausea and vomiting (PONV) and frequency of the need for antiemetic therapy were recorded. Primary study outcome was the ability of the study infusions to reduce consumption of PO pethidine down to one dose during 24-hr PO.
IO use of REMI or DEX infusion allowed hemodynamic control to surgical stresses with nonsignificant difference between both infusions. REMI infusion insured significantly rapid recovery and short OR times but required larger volume of sevoflurane during surgery and proper PO follow-up for pain and PONV. DEX infusion significantly improved control of PO pain with a larger number of patient requested rescue analgesia only once, reduced the dose of PO analgesia, reduced the frequency of PONV, and the need for antiemetic therapy.
REMI or DEX infusion as IO adjuvant to general anesthesia is appropriate option to achieve hemodynamic control of surgical stresses and to improve perioperative outcomes. REMI infusion may be preferred for its induced rapid recovery and short OR time, whereas DEX infusion may be chosen for its improved control of PO pain and reduction of PO analgesia and frequency of PONV.
评估在腹腔镜胃袖状切除术的七氟醚麻醉期间,术中输注右美托咪定(DEX)与瑞芬太尼(REMI)相比的术后(PO)镇痛效果。
132例体重指数>35kg·m且美国麻醉医师协会(ASA)分级为II或III级的患者,随机分为R组,气管插管后接受瑞芬太尼输注(6 - 18μg·kg·h),D组接受右美托咪定输注(0.2 - 0.5μg·kg·h),直至吸入麻醉停止前。手术期间及术后无创监测心率和平均动脉压。记录苏醒时间、直至转入麻醉后护理单元的时间以及总手术室(OR)时间。记录术后肩尖痛和伤口疼痛评分,并给予50mg哌替啶肌肉注射进行补救镇痛。记录术后恶心呕吐(PONV)的发生情况以及抗呕吐治疗的需求频率。主要研究结果是研究输注在术后24小时内将哌替啶的使用量减少至一剂的能力。
术中使用瑞芬太尼或右美托咪定输注可实现对手术应激的血流动力学控制,两种输注之间无显著差异。瑞芬太尼输注确保了显著更快的恢复和更短的手术室时间,但手术期间需要更大剂量的七氟醚,且术后需对疼痛和PONV进行适当随访。右美托咪定输注显著改善了术后疼痛控制,更多患者仅需一次补救镇痛,减少了术后镇痛剂量,降低了PONV的频率以及抗呕吐治疗的需求。
瑞芬太尼或右美托咪定输注作为全身麻醉的术中辅助用药,是实现对手术应激的血流动力学控制并改善围手术期结局的合适选择。瑞芬太尼输注因其诱导快速恢复和缩短手术室时间可能更受青睐,而右美托咪定输注因其改善术后疼痛控制、减少术后镇痛和PONV频率可能被选用。