Abdulghani Mohanad Mundher, Abbas Mohamad Natiq, Mohammed Wafaa Redha
Al-Kindy College of Medicine Baghdad, University of Baghdad, Baghdad, Iraq.
Open Access Maced J Med Sci. 2019 Oct 11;7(21):3514-3520. doi: 10.3889/oamjms.2019.751. eCollection 2019 Nov 15.
Diffuse astrocytomas constitute the largest group of primary malignant human intracranial tumours. They are classified by the World Health Organization (WHO) into three histological malignancy grades: diffuse astrocytomas (grade II), anaplastic astrocytomas (grade III) and glioblastoma (grade IV) based on histopathological features such as cellular atypia, mitotic activity, necrosis and microvascular proliferation. Epidermal growth factor receptor (EGFR) is a 170-kDa transmembrane tyrosine kinase receptor expressed in a variety of normal and malignant cells regulating critical cellular processes. When activated, epidermal growth factor receptor (EGFR) triggers several signalling cascades leading to increased proliferation and angiogenesis and decreased apoptosis and hence associated with aggressive progression of the tumour. Epidermal growth factor receptor (EGFR) level is known to be a strong indicator associated with the aggressive behaviour of the tumour and acts as a prognostic factor for evaluating the survival rate.
To evaluate the expression of epidermal growth factor receptor (EGFR) in different grades of astrocytoma.
formalin-fixed paraffin-embedded astrocytic tumours of 44 patients were collected from the archival material of pathology department of Ghazi Al Hariri Teaching Hospital during the period from June to December 2018. Hematoxylin and eosin-stained sections were used to characterise the tumours histologically based on cellularity, nuclear hyperchromasia, polymorphism, mitotic activity, vascular proliferation and necrosis with or without pseudopallisading of tumour cells. Diagnosis and grading of astrocytic tumours in this study were made according to WHO criteria (2016). Using a monoclonal antibody to the epidermal growth factor receptor (EGFR) and immunohistochemical analysis, the expression and distribution of epidermal growth factor receptor in astrocytic tumours were examined.
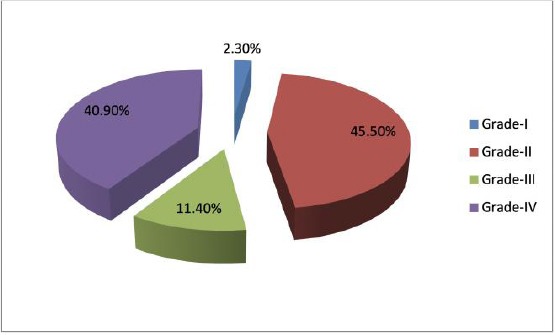
The study included 1 case pilocytic astrocytoma (grade I), 20 cases diffuse astrocytoma (grade II), 5 cases anaplastic astrocytoma (grade III) and 18 cases of glioblastoma (grade IV). Expression of EGFR was found in 38.88% of the glioblastoma samples (grade IV). However, none of the astrocytomas of WHO grades I, II and III showed immunoreactivity for EGFR protein. Different patterns of immunoreactive cells and significant intratumor heterogeneity of EGFR expression were observed in glioblastomas.
The immunohistochemical expression of Epidermal growth factor receptor (EGFR) was restricted only to high-grade astrocytic tumours, namely glioblastoma, thus may use to predict glioblastoma.
弥漫性星形细胞瘤是原发性人类恶性颅内肿瘤中最大的一组。世界卫生组织(WHO)根据细胞异型性、有丝分裂活性、坏死和微血管增殖等组织病理学特征,将它们分为三个组织学恶性等级:弥漫性星形细胞瘤(二级)、间变性星形细胞瘤(三级)和胶质母细胞瘤(四级)。表皮生长因子受体(EGFR)是一种170 kDa的跨膜酪氨酸激酶受体,在多种正常和恶性细胞中表达,调节关键的细胞过程。激活后,表皮生长因子受体(EGFR)触发多个信号级联反应,导致增殖增加和血管生成增加,凋亡减少,因此与肿瘤的侵袭性进展相关。已知表皮生长因子受体(EGFR)水平是与肿瘤侵袭性相关的一个重要指标,并且作为评估生存率的一个预后因素。
评估表皮生长因子受体(EGFR)在不同等级星形细胞瘤中的表达。
2018年6月至12月期间,从加齐·哈里里教学医院病理科存档材料中收集44例患者的福尔马林固定石蜡包埋星形细胞瘤。苏木精和伊红染色切片用于根据细胞密度、核深染、多形性、有丝分裂活性、血管增殖以及有无肿瘤细胞假栅栏状坏死对肿瘤进行组织学特征分析。本研究中星形细胞瘤的诊断和分级根据WHO标准(2016年)进行。使用针对表皮生长因子受体(EGFR)的单克隆抗体和免疫组织化学分析,检测表皮生长因子受体在星形细胞瘤中的表达和分布。
该研究包括1例毛细胞型星形细胞瘤(一级)、20例弥漫性星形细胞瘤(二级)、5例间变性星形细胞瘤(三级)和18例胶质母细胞瘤(四级)。在38.88%的胶质母细胞瘤样本(四级)中发现了EGFR的表达。然而,WHO一级、二级和三级星形细胞瘤均未显示EGFR蛋白免疫反应性。在胶质母细胞瘤中观察到免疫反应性细胞的不同模式以及EGFR表达的显著肿瘤内异质性。
表皮生长因子受体(EGFR)的免疫组织化学表达仅局限于高级别星形细胞瘤,即胶质母细胞瘤,因此可用于预测胶质母细胞瘤。