Breilh Dominique, Honore Patrick M, De Bels David, Roberts Jason A, Gordien Jean Baptiste, Fleureau Catherine, Dewitte Antoine, Coquin Julien, Rozé Hadrien, Perez Paul, Attou Rachid, Redant Sebastien, Kugener Luc, Saux Marie-Claude, Spapen Herbert D, Ouattara Alexandre, Joannes-Boyau Olivier
Laboratory of Clinical Pharmacokinetics and Clinical Pharmacy, INSERM U1034, Haut-Lévêque Hospital, CHU Bordeaux, University of Bordeaux, Segalen, Pessac, France.
Intensive Care Department, Centre Hospitalier Universitaire Brugmann-Brugmann University Hospital, Brussels, Belgium.
J Transl Int Med. 2019 Dec 31;7(4):155-169. doi: 10.2478/jtim-2019-0031. eCollection 2019 Dec.
Hemofiltration rate, changes in blood and ultrafiltration flow, and discrepancies between the prescribed and administered doses strongly influence pharmacokinetics (PK) and pharmacodynamics (PD) of antimicrobial agents during continuous veno-venous hemofiltration (CVVH) in critically ill patients.
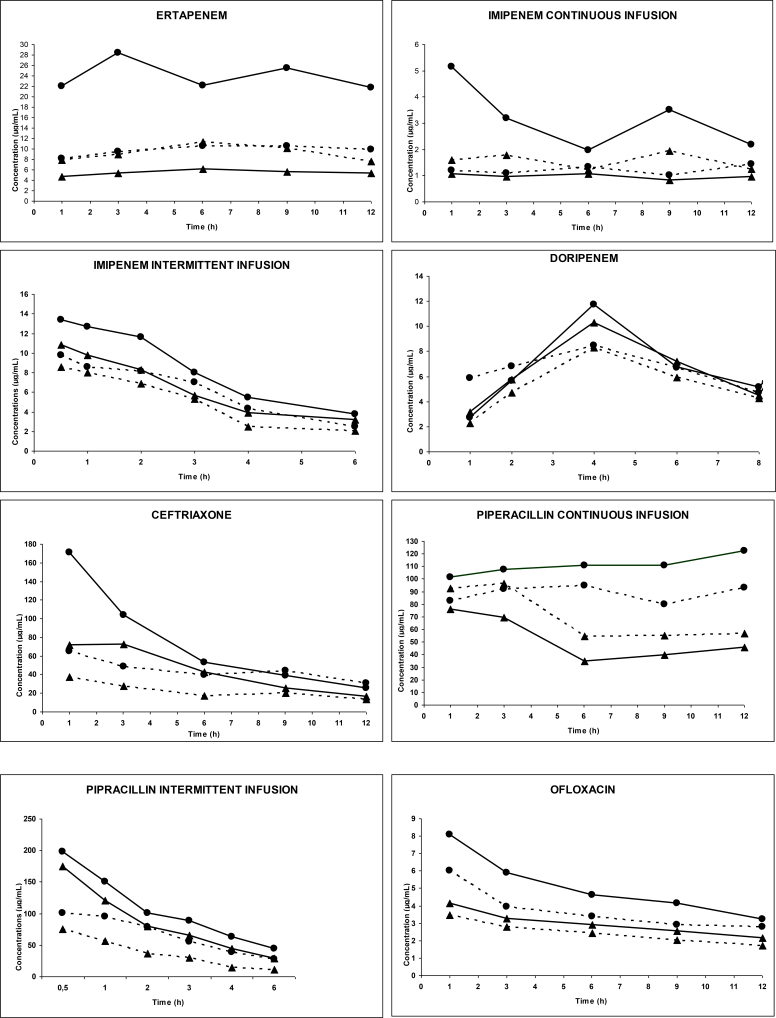
Ancillary data were from the prospective multicenter IVOIRE (hIgh VOlume in Intensive caRE) study. High volume (HV, 70 mL/kg/h) was at random compared with standard volume (SV, 35 mL/kg/h) CVVH in septic shock patients with acute kidney injury (AKI). PK/PD parameters for all antimicrobial agents used in each patient were studied during five days.
Antimicrobial treatment met efficacy targets for both percentage of time above the minimal inhibitory concentration and inhibitory quotient. A significant correlation was observed between the ultrafiltration flow and total systemic clearance (Spearman test: < 0.005) and between CVVH clearance and drug elimination half-life (Spearman test: < 0.005). All agents were easily filtered. Mean sieving coefficient ranged from 38.7% to 96.7%. Mean elimination half-life of all agents was significantly shorter during HV-CVVH (from 1.29 to 28.54 h) than during SV-CVVH (from 1.51 to 33.85 h) ( < 0.05).
This study confirms that CVVH influences the PK/PD behavior of most antimicrobial agents. Antimicrobial elimination was directly correlated with convection rate. Current antimicrobial dose recommendations will expose patients to underdosing and increase the risk for treatment failure and development of resistance. Dose recommendations are proposed for some major antibiotic and antifungal treatments in patients receiving at least 25 mL/kg/h CVVH.
在危重症患者的持续静脉-静脉血液滤过(CVVH)过程中,血液滤过率、血液和超滤流量的变化以及规定剂量与实际给药剂量之间的差异,强烈影响抗菌药物的药代动力学(PK)和药效学(PD)。
辅助数据来自前瞻性多中心IVOIRE(重症监护中的高容量)研究。在患有急性肾损伤(AKI)的感染性休克患者中,将高容量(HV,70 mL/kg/h)与标准容量(SV,35 mL/kg/h)CVVH进行随机比较。在五天内研究了每位患者使用的所有抗菌药物的PK/PD参数。
抗菌治疗达到了高于最低抑菌浓度的时间百分比和抑制商的疗效目标。超滤流量与总全身清除率之间(Spearman检验:<0.005)以及CVVH清除率与药物消除半衰期之间(Spearman检验:<0.005)观察到显著相关性。所有药物都易于滤过。平均筛系数范围为38.7%至96.7%。与SV-CVVH期间(1.51至33.85小时)相比,所有药物在HV-CVVH期间的平均消除半衰期均显著缩短(从1.29至28.54小时)(<0.05)。
本研究证实CVVH会影响大多数抗菌药物的PK/PD行为。抗菌药物的清除与对流率直接相关。当前的抗菌药物剂量建议会使患者用药不足,并增加治疗失败和耐药性发展的风险。针对接受至少25 mL/kg/h CVVH的患者,提出了一些主要抗生素和抗真菌治疗的剂量建议。