van Riet Priscilla A, Quispel Rutger, Cahen Djuna L, Snijders-Kruisbergen Mieke C, van Loenen Petri, Erler Nicole S, Poley Jan-Werner, van Driel Lydi M J W, Mulder Sanna A, Veldt Bart J, Leeuwenburgh Ivonne, Anten Marie-Paule G F, Honkoop Pieter, Thijssen Annemieke Y, Hol Lieke, Hadithi Mohammed, Fitzpatrick Claire E, Schot Ingrid, Bergmann Jilling F, Bhalla Abha, Bruno Marco J, Biermann Katharina
Department of Gastroenterology, Erasmus MC University Medical Center Rotterdam, the Netherlands.
Deparment of Gastroenterology and Hepatology, Reinier de Graaf Hospital, Delft, the Netherlands.
Endosc Int Open. 2020 Feb;8(2):E155-E162. doi: 10.1055/a-1038-4103. Epub 2020 Jan 22.
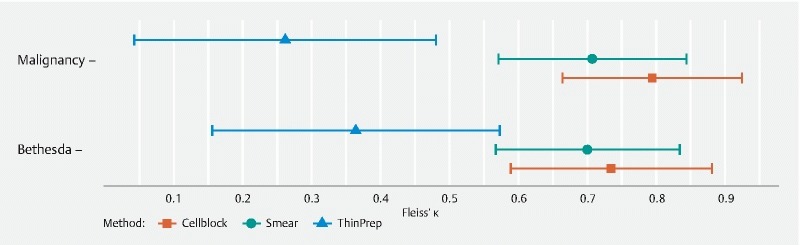
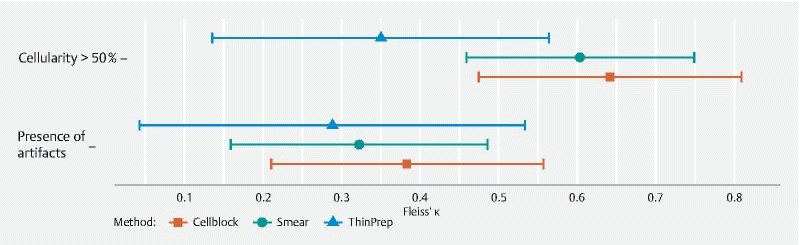
The traditional "smear technique" for processing and assessing endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) is sensitive to artifacts. Processing and evaluation of specimens collected in a liquid medium, liquid-based cytology (LBC) may be a solution. We compared the diagnostic value of EUS-FNA smears to LBC in pancreatic solid lesions in the absence of rapid on-site evaluation (ROSE). Consecutive patients who required EUS-FNA of a solid pancreatic lesion were included in seven hospitals in the Netherlands and followed for at least 12 months. Specimens from the first pass were split into two smears and a vial for LBC (using ThinPrep and/or Cell block). Smear and LBC were compared in terms of diagnostic accuracy for malignancy, sample quality, and diagnostic agreement between three cytopathologists. Diagnostic accuracy for malignancy was higher for LBC (82 % (58/71)) than for smear (66 % (47/71), = 0.04), but did not differ when smears were compared to ThinPrep (71 % (30/42), = 0.56) or Cell block (62 % (39/63), = 0.61) individually. Artifacts were less often present in ThinPrep (57 % (24/42), = 0.02) or Cell block samples (40 % (25/63), < 0.001) than smears (76 % (54/71)). Agreement on malignancy was equally good for smears and LBC (ĸ = 0.71 versus ĸ = 0.70, = 0.98), but lower for ThinPrep (ĸ = 0.26, = 0.01) than smears. After a single pass, LBC provides higher diagnostic accuracy than the conventional smear technique for EUS-FNA of solid pancreatic lesions in the absence of ROSE. Therefore, LBC, may be an alternative to the conventional smear technique, especially in centers lacking ROSE.
用于处理和评估超声内镜引导下细针穿刺活检(EUS-FNA)标本的传统“涂片技术”对伪像敏感。在液体培养基中收集标本并进行处理和评估,液基细胞学(LBC)可能是一种解决方案。我们比较了在没有快速现场评估(ROSE)的情况下,EUS-FNA涂片与LBC对胰腺实性病变的诊断价值。荷兰七家医院纳入了需要对胰腺实性病变进行EUS-FNA的连续患者,并对其进行了至少12个月的随访。首次穿刺获得的标本被分成两张涂片和一个用于LBC的小瓶(使用ThinPrep和/或细胞块)。比较了涂片和LBC在恶性肿瘤诊断准确性、样本质量以及三位细胞病理学家之间的诊断一致性方面的差异。LBC对恶性肿瘤的诊断准确性(82%(58/71))高于涂片(66%(47/71),P = 0.04),但当将涂片分别与ThinPrep(71%(30/42),P = 0.56)或细胞块(62%(39/63),P = 0.61)比较时,差异无统计学意义。ThinPrep(57%(24/42),P = 0.02)或细胞块样本(40%(25/63),P < 0.001)中出现伪像的频率低于涂片(76%(54/71))。涂片和LBC在恶性肿瘤诊断上的一致性同样良好(κ = 0.71对κ = 0.70,P = 0.98),但ThinPrep(κ = 0.26,P = 0.01)与涂片相比一致性较低。在单次穿刺后,对于没有ROSE的胰腺实性病变的EUS-FNA,LBC比传统涂片技术具有更高的诊断准确性。因此,LBC可能是传统涂片技术的一种替代方法,尤其是在缺乏ROSE的中心。