Bazarbashi Ahmad Najdat, Wang Thomas J, Thompson Christopher C, Ryou Marvin
Division of Gastroenterology, Hepatology and Endoscopy. Brigham and Women's Hospital, Boston, Massachusetts, United States.
Harvard Medical School, Boston, Massachusetts, United States.
Endosc Int Open. 2020 Feb;8(2):E221-E227. doi: 10.1055/a-1027-6708. Epub 2020 Jan 28.
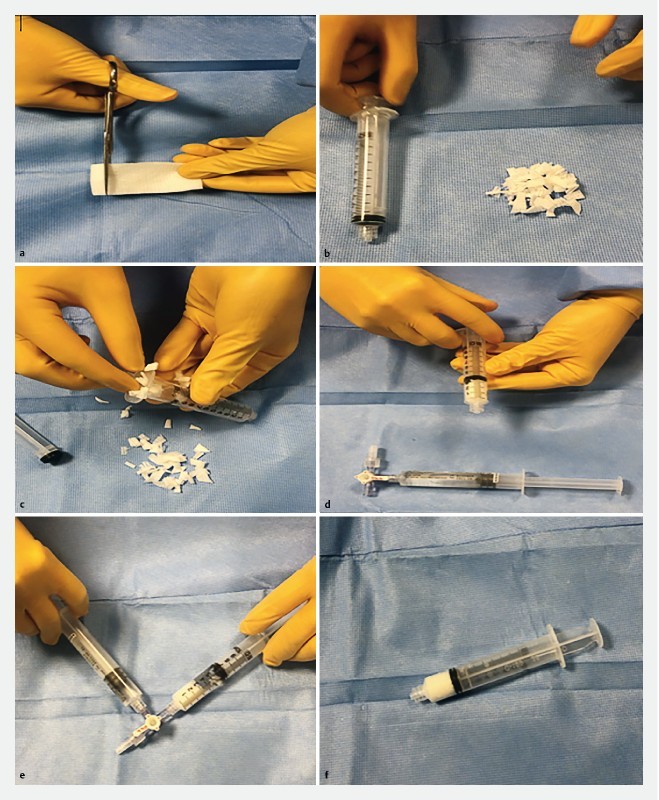
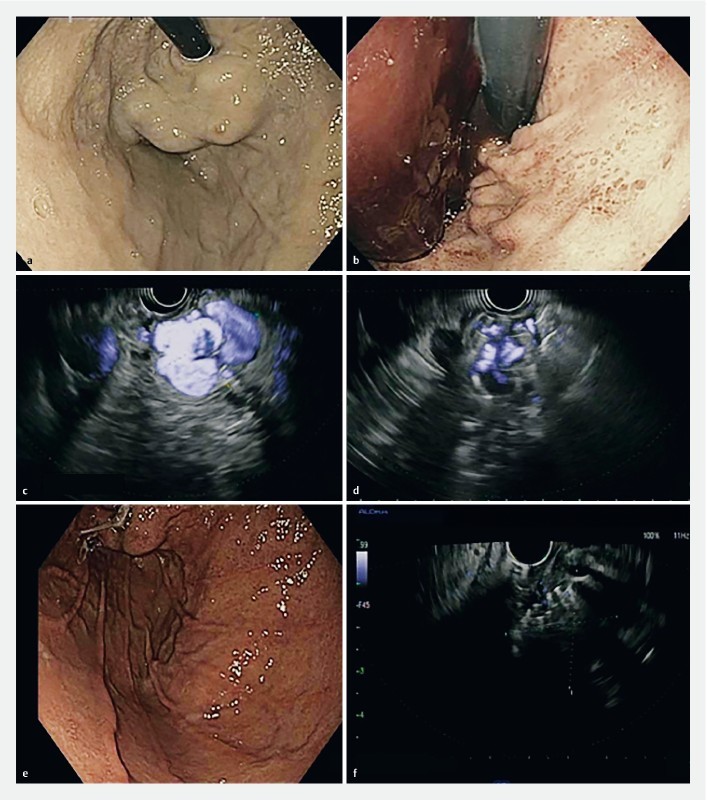
Bleeding from gastric varices (GV) carries high morbidity and mortality. Current endoscopic therapies are premised on cyanoacrylate injection which is technically challenging and carries risk of embolization. We present a case series of endoscopic ultrasound (EUS)-guided coil injection in combination with hemostatic absorbable gelatin sponge (AGS) for treatment of bleeding gastric varices. This was a retrospective review of EUS-guided coil injection for bleeding GV since November 2017. After EUS-guided needle puncture, hemostatic coils were serially injected until significant reduction of Doppler flow. Under fluoroscopic guidance, test contrast was injected to confirm absence of run-off, at which time AGS, converted into a liquid slurry, was injected as hemostatic reinforcement. Ten consecutive patients underwent EUS-guided coil embolization reinforced by AGS. Technical success, defined as uncomplicated injection of coils and sponge was achieved in 100 % (10/10). Mean follow-up was 6 months 73-397 days; No patients rebled or required reintervention on GV. The complication rate was 10 % (1/10; severe abdominal pain without radiographic findings); otherwise, there were no cases of systemic embolization. Nine of 10 patients (90 %) had follow-up EUS (mean 80 days); 100 % (9/9) revealed near-obliteration of GV. EUS-guided coil embolization in combination with hemostatic AGS is a novel method for management of bleeding GV with high clinical and technical success rates, low risk for complications and favorable safety profile when compared to cyanoacrylate. This technique theoretically minimizes embolic complications and need for re-intervention. Further studies are required to compare this modality.
胃静脉曲张(GV)出血的发病率和死亡率很高。目前的内镜治疗以氰基丙烯酸酯注射为基础,这在技术上具有挑战性且有栓塞风险。我们报告了一系列内镜超声(EUS)引导下线圈注射联合可吸收止血明胶海绵(AGS)治疗胃静脉曲张出血的病例。
这是一项对2017年11月以来EUS引导下线圈注射治疗出血性GV的回顾性研究。在EUS引导下进行针穿刺后,连续注射止血线圈,直到多普勒血流显著减少。在荧光透视引导下,注射试验性造影剂以确认无造影剂外溢,此时将转化为液体浆状的AGS作为止血强化剂注射。
连续10例患者接受了EUS引导下由AGS强化的线圈栓塞术。技术成功率定义为顺利注射线圈和海绵,为100%(10/10)。平均随访6个月(73 - 397天);没有患者再次出血或需要对GV进行再次干预。并发症发生率为10%(1/10;严重腹痛但无影像学表现);此外,没有全身栓塞的病例。10例患者中有9例(90%)接受了随访EUS(平均80天);100%(9/9)显示GV几乎闭塞。
与氰基丙烯酸酯相比,EUS引导下线圈栓塞联合止血AGS是一种治疗出血性GV的新方法,具有较高的临床和技术成功率、较低的并发症风险和良好的安全性。该技术理论上可将栓塞并发症和再次干预的需求降至最低。需要进一步研究来比较这种治疗方式。