Bazarbashi Ahmad Najdat, Wang Thomas J, Jirapinyo Pichamol, Thompson Christopher C, Ryou Marvin
Division of Gastroenterology, Hepatology and Endoscopy, Brigham and Women's Hospital, Boston, Massachusetts, USA.
Department of Internal Medicine, Massachusetts General Hospital, Boston, Massachusetts, USA.
Clin Transl Gastroenterol. 2020 May;11(5):e00175. doi: 10.14309/ctg.0000000000000175.
Gastric variceal (GV) bleeding is a feared complication of cirrhosis. Traditional endoscopic treatment with cyanoacrylate (CYA) injection can be challenging. Alternatively, endoscopic ultrasound (EUS)-guided delivery of hemostatic coils has shown high therapeutic success without the complications profile of CYA alone. Our aim was to compare the clinical outcomes of EUS-guided coil embolization with endoscopic CYA injection for the treatment of GV.
We performed a matched cohort study using a prospective registry involving 2 tertiary centers. A total of 10 patients undergoing EUS-based coil therapy were matched in 1:3 fashion to 30 patients who underwent CYA injection. The matching criteria included type of GV, Charlson comorbidity index, and bleeding severity. Primary outcomes were technical success and complications. Secondary outcomes were rebleeding rates, reinterventions rates, total transfusion requirements, and time-to-event analysis (rebleeding, reintervention, and transfusion).
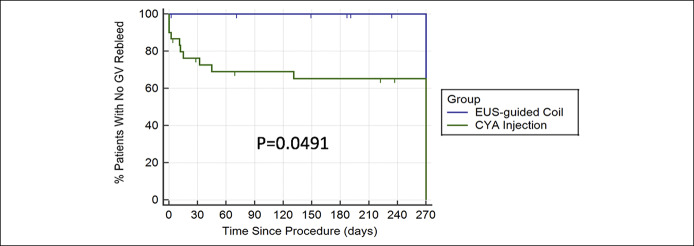
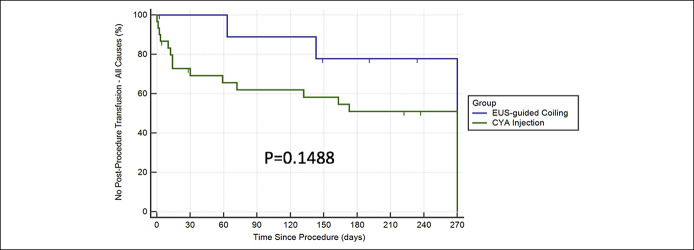
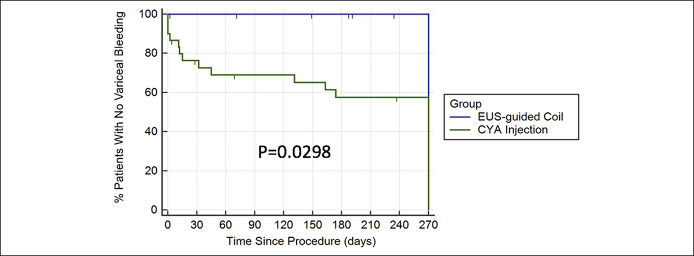
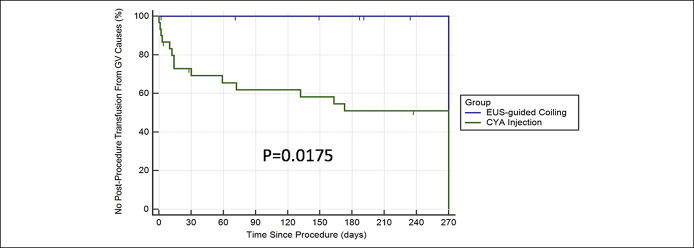
Technical success was 100% for EUS coil therapy vs 96.7% for CYA injection (P = 1.0). Complication rates were 10% in the EUS coil group vs 20% in the CYA group; P = 0.65. At 9 months, no EUS coil patient had rebled compared with 38% of the CYA group. No EUS coil patient required blood transfusion for GV rebleed, whereas over 50% of CYA patients did. Ten percent of EUS coil patients required reintervention compared with 60% of CYA patients. The EUS coil group had superior time to reintervention, GV rebleed, and transfusions (all P < 0.05).
Compared with CYA, EUS-guided coil injection appears superior for the treatment of GV and should be considered initial endoscopic treatment of choice in centers with interventional EUS expertise.
胃静脉曲张(GV)出血是肝硬化令人恐惧的并发症。传统的内镜下用氰基丙烯酸酯(CYA)注射治疗可能具有挑战性。另外,内镜超声(EUS)引导下输送止血线圈已显示出较高的治疗成功率,且没有单独使用CYA的并发症。我们的目的是比较EUS引导下线圈栓塞术与内镜下CYA注射治疗GV的临床结果。
我们使用前瞻性登记系统进行了一项匹配队列研究,涉及2个三级中心。总共10例接受基于EUS的线圈治疗的患者与30例接受CYA注射的患者以1:3的方式进行匹配。匹配标准包括GV类型、Charlson合并症指数和出血严重程度。主要结局是技术成功率和并发症。次要结局是再出血率、再次干预率、总输血需求量以及事件发生时间分析(再出血、再次干预和输血)。
EUS线圈治疗的技术成功率为100%,而CYA注射为96.7%(P = 1.0)。EUS线圈组的并发症发生率为10%,而CYA组为20%;P = 0.65。在9个月时,没有EUS线圈治疗的患者发生再出血,而CYA组为该比例为38%。没有EUS线圈治疗的患者因GV再出血需要输血,而超过50%的CYA患者需要输血。10%的EUS线圈治疗患者需要再次干预,而CYA患者为60%。EUS线圈组在再次干预、GV再出血和输血的时间方面表现更优(所有P < 0.05)。
与CYA相比,EUS引导下线圈注射在治疗GV方面似乎更具优势,在具有介入性EUS专业知识的中心应被视为内镜治疗的首选。