Kusakabe Jiro, Hata Koichiro, Tanaka Shiro, Omae Katsuhiro, Okamura Yusuke, Tajima Tetsuya, Tamaki Ichiro, Miyauchi Hidetaka, Kubota Toyonari, Tanaka Hirokazu, Uemoto Shinji
Department of Surgery, Division of Hepato-Biliary-Pancreatic Surgery and Transplantation, Kyoto University Graduate School of Medicine, Kyoto, Japan.
Department of Clinical Biostatistics, Kyoto University Graduate School of Medicine, Kyoto, Japan.
Hepatol Res. 2020 Jun;50(6):741-753. doi: 10.1111/hepr.13489. Epub 2020 Feb 18.
Six-month recipient mortality after adult-to-adult living-donor liver transplantation (LDLT) remains high. Early and accurate prediction of recipient outcome and continuous monitoring of recipient severity after surgery are both essential for guiding appropriate care. This study was designed to identify early post-transplant parameters associated with 6-month mortality, and thereby to construct a discriminatory prognostic index (PI).
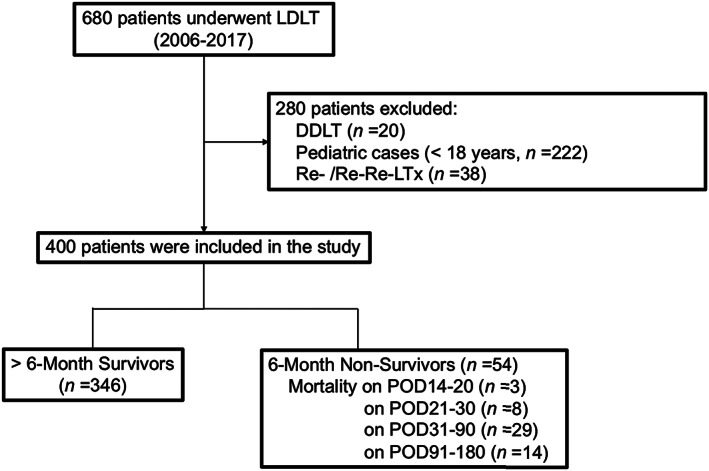
We retrospectively analyzed 400 consecutive primary adult-to-adult LDLTs in our center (2006-2017). Perioperative variables were comprehensively analyzed for their accuracy in predicting recipient mortality by comparing the area under the receiver operating characteristic (AUROC) of each factor.
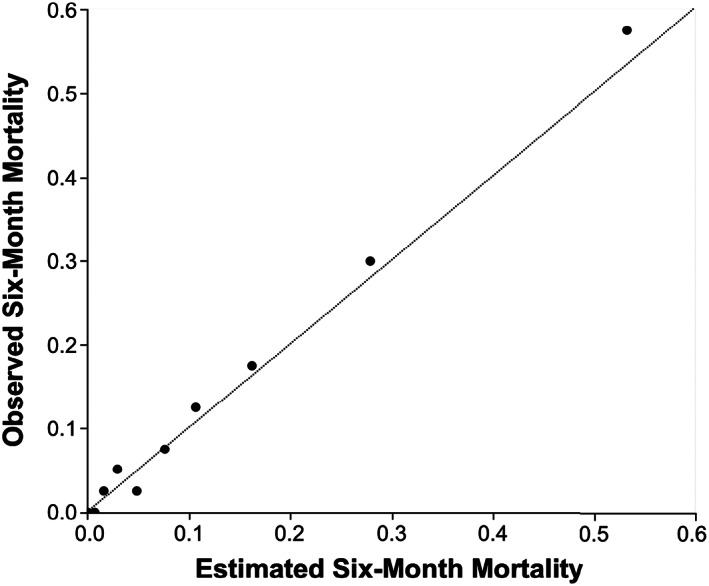
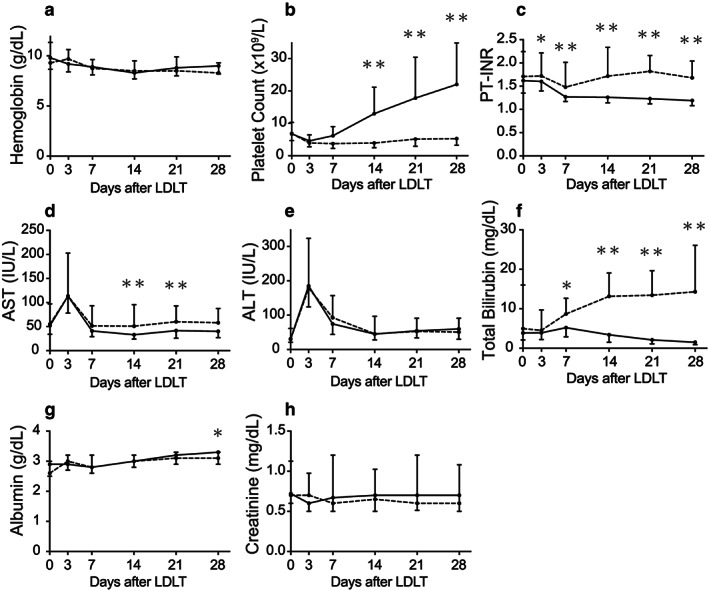
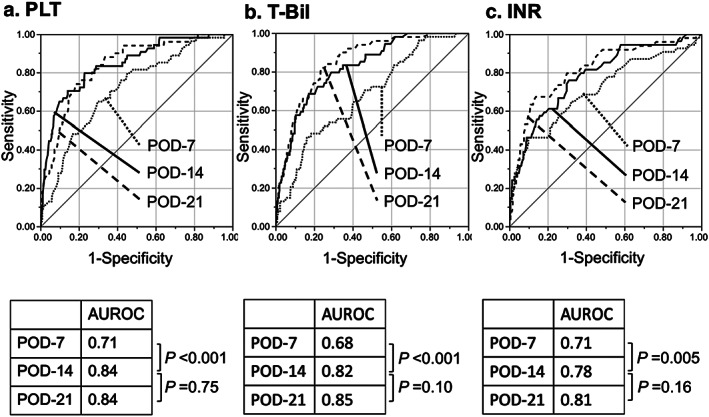
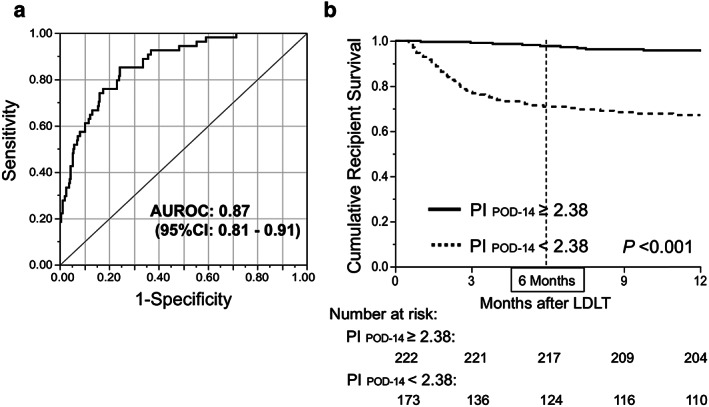
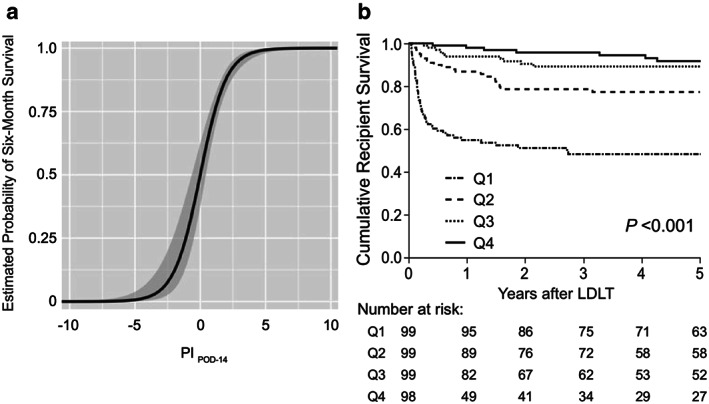
The AUROCs of preoperative predictive factors, for example, Model for End-stage Liver Disease (MELD) score and donor age, were 0.56 and 0.64, respectively, whereas those of post-transplant platelet count (PLT), total bilirubin (T-BIL), and prothrombin time - international normalized ratio (INR) on postoperative day (POD)-7-14 were 0.71/0.84, 0.68/0.82, and 0.71/0.78, respectively. Logistic regression analysis provided a formula: PI = 3.39 + 0.12 × PLT - 0.09 × T-BIL - 1.23 × INR , indicating a high AUROC of 0.87. Recipient 6-month survival with PI < 2.38 (n = 173) was 71.7%, whereas that with PI ≥ 2.38 (n = 222) was 97.7% (P < 0.001). The AUROCs of PI were as high as 0.8 in the subgroups with younger donors (<50 years of age), right lobe grafts, ABO-identical/compatible combinations, or low MELD score (<20), indicating usefulness of PI to identify unexpectedly complicated cases within the first week.
A novel, post-transplant survival estimator, PI, accurately predicts recipient 6-month mortality within 1-2 weeks after adult LDLT. Daily monitoring of PI could facilitate early interventions including retransplantation in critically ill patients.
成人活体肝移植(LDLT)术后6个月受者死亡率仍然很高。早期准确预测受者预后以及术后持续监测受者病情严重程度对于指导恰当治疗均至关重要。本研究旨在识别与6个月死亡率相关的移植后早期参数,从而构建一个具有鉴别能力的预后指数(PI)。
我们回顾性分析了本中心400例连续的成人对成人原发性LDLT病例(2006 - 2017年)。通过比较各因素的受试者工作特征曲线下面积(AUROC),全面分析围手术期变量预测受者死亡率的准确性。
术前预测因素,如终末期肝病模型(MELD)评分和供体年龄的AUROC分别为0.56和0.64,则术后第7 - 14天的移植后血小板计数(PLT)、总胆红素(T - BIL)和凝血酶原时间 - 国际标准化比值(INR)的AUROC分别为0.71/0.84、0.68/0.82和0.71/0.78。逻辑回归分析得出公式:PI = 3.39 + 0.12×PLT - 0.09×T - BIL - 1.23×INR,显示AUROC为0.87。PI<2.38(n = 173)的受者6个月生存率为71.7%,而PI≥2.38(n = 222)的受者6个月生存率为97.7%(P<0.001)。在供体较年轻(<50岁)、右叶移植、ABO血型相同/相容组合或MELD评分较低(<20)的亚组中,PI的AUROC高达0.8,表明PI有助于在第一周内识别意外复杂的病例。
一种新的移植后生存估计指标PI,能在成人LDLT术后1 - 2周内准确预测受者6个月死亡率。每日监测PI有助于早期干预,包括对重症患者进行再次移植。