Privé Bastiaan, Kortleve Michael, van Basten Jean-Paul
Department of Urology, Canisius Wilhelmina Hospital, Nijmegen, The Netherlands.
Department of Urology, Hospital Gelderse Vallei, Ede, The Netherlands.
Cent European J Urol. 2019;72(4):369-373. doi: 10.5173/ceju.2019.0021. Epub 2019 Nov 14.
Laparoscopic nephrectomy (LN) is the most performed laparoscopic procedure by urologic residents (Res). A large amount of data exists on laparoscopic nephrectomies in terms of safety and surgical outcomes, but only a little is known about the influence of residents. The purpose of this study was to evaluate this influence on the clinical outcome of a laparoscopic nephrectomy.
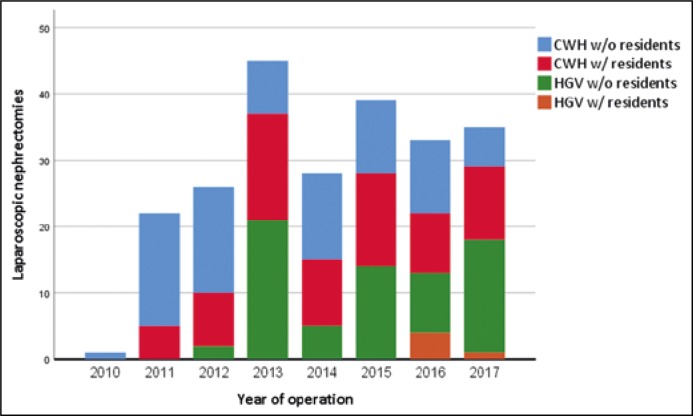
Retrospectively, patients who had undergone a LN between 2010 and 2018 were assessed. Data included patient demographics, date of surgery, pre- and postoperative results and complications. The patients who had undergone a LN were divided into two groups: one where residents were involved and another group where only a staff surgeon (Sur) performed the operation. All training residents had a questionnaire sent to them to evaluate their role during the LN.
A total of 229 patients met the study criteria, of which 78 patients were operated together with a resident and 151 by a staff surgeon alone. Both groups were homogeneous in terms of age, comorbidities, left/right sided LN and tumor-stage. Between these two groups, no significant differences were observed in median estimated blood loss (Res 87 ml vs. Sur 100 ml), intraoperative adverse events (Res 10.3% vs. Sur 6% p = 0.24), conversion to open surgery (Res 6.4% vs. Sur 6%) and high-grade postoperative complications (Res 3.9% vs. Sur 4.6%). However, when a resident participated, the LN lasted on average 20 minutes longer (Res mean 130 min vs. Sur 110 min p ≤0.001).
Our data shows that involvement of a resident in laparoscopic nephrectomy has no effect on the clinical outcome. Therefore, it is safe to perform a laparoscopic nephrectomy together with a resident, but it is important to take the additional surgical time into account.
腹腔镜肾切除术(LN)是泌尿外科住院医师(Res)实施最多的腹腔镜手术。关于腹腔镜肾切除术的安全性和手术结果已有大量数据,但对于住院医师的影响却知之甚少。本研究的目的是评估这种影响对腹腔镜肾切除术临床结果的作用。
回顾性评估2010年至2018年间接受LN手术的患者。数据包括患者人口统计学信息、手术日期、术前和术后结果及并发症。接受LN手术的患者分为两组:一组有住院医师参与,另一组仅由主治医生(Sur)实施手术。所有参与培训的住院医师都收到一份问卷,以评估他们在LN手术中的作用。
共有229例患者符合研究标准,其中78例患者与住院医师一起手术,151例仅由主治医生单独手术。两组在年龄、合并症、左右侧LN及肿瘤分期方面具有同质性。在这两组之间,中位估计失血量(住院医师组87毫升 vs. 主治医生组100毫升)、术中不良事件(住院医师组10.3% vs. 主治医生组6%,p = 0.24)、转为开放手术(住院医师组6.4% vs. 主治医生组6%)和高级别术后并发症(住院医师组3.9% vs. 主治医生组4.6%)方面均未观察到显著差异。然而,当有住院医师参与时,LN手术平均持续时间长20分钟(住院医师组平均130分钟 vs. 主治医生组110分钟,p≤0.001)。
我们的数据表明,住院医师参与腹腔镜肾切除术对临床结果没有影响。因此,与住院医师一起进行腹腔镜肾切除术是安全的,但考虑到额外的手术时间很重要。