Franchineau Guillaume, Bréchot Nicolas, Hekimian Guillaume, Lebreton Guillaume, Bourcier Simon, Demondion Pierre, Le Guennec Loïc, Nieszkowska Ania, Luyt Charles-Edouard, Combes Alain, Schmidt Matthieu
INSERM, UMRS_1166-iCAN, Institute of Cardiometabolism and Nutrition, Sorbonne Universités, UPMC Univ Paris 06, 75651, Paris Cedex 13, France.
Medical Intensive Care Unit, Assistance Publique-Hôpitaux de Paris, Pitié-Salpêtrière Hospital, 75651, Paris Cedex 13, France.
Ann Intensive Care. 2020 Feb 3;10(1):12. doi: 10.1186/s13613-020-0633-5.
Prone positioning (PP) during veno-venous ECMO is feasible, but its physiological effects have never been thoroughly evaluated. Our objectives were to describe, through electrical impedance tomography (EIT), the impact of PP on global and regional ventilation, and optimal PEEP level.
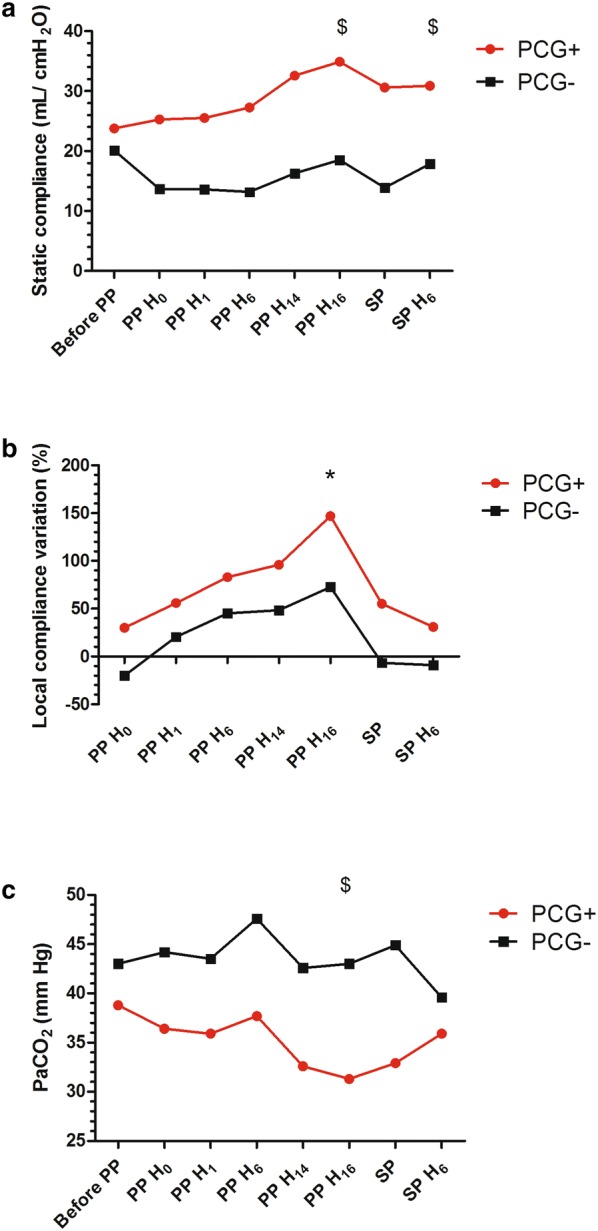
A monocentric study conducted on ECMO-supported severe ARDS patients, ventilated in pressure-controlled mode, with 14-cmHO driving pressure and EIT-based "optimal PEEP". Before, during and after a 16-h PP session, EIT-based distribution and variation of tidal impedance, VT/VT ratio, end-expiratory lung impedance (EELI) and static compliance were collected. Subgroup analyses were performed in patients who increased their static compliance by ≥ 3 mL/cmHO after 16 h of PP.
For all patients (n = 21), tidal volume and EELI were redistributed from ventral to dorsal regions during PP. EIT-based optimal PEEP was significantly lower in PP than in supine position. Median (IQR) optimal PEEP decreased from 14 (12-16) to 10 (8-14) cmHO. Thirteen (62%) patients increased their static compliance by ≥ 3 mL/cmHO after PP on ECMO. This subgroup had higher body mass index, more frequent viral pneumonia, shorter ECMO duration, and lower baseline VT/VT ratio than patients with compliance ≤ 3 mL/cmHO (P < 0.01).
Although baseline tidal volume distribution on EIT may predict static compliance improvement after PP on ECMO, our results support physiological benefits of PP in all ECMO patients, by modifying lung mechanics and potentially reducing VILI. Further studies, including a randomized-controlled trial, are now warranted to confirm potential PP benefits during ECMO.
静脉-静脉体外膜肺氧合(ECMO)期间的俯卧位通气(PP)是可行的,但其生理效应尚未得到全面评估。我们的目标是通过电阻抗断层扫描(EIT)描述PP对整体和局部通气以及最佳呼气末正压(PEEP)水平的影响。
对接受ECMO支持的重症急性呼吸窘迫综合征(ARDS)患者进行单中心研究,这些患者采用压力控制模式通气,驱动压力为14 cmH₂O,并基于EIT设置“最佳PEEP”。在16小时的PP疗程之前、期间和之后,收集基于EIT的潮气量阻抗分布和变化、潮气量/预测潮气量比值(VT/VT ratio)、呼气末肺阻抗(EELI)和静态顺应性。对PP 16小时后静态顺应性增加≥3 mL/cmH₂O的患者进行亚组分析。
对于所有患者(n = 21),PP期间潮气量和EELI从腹侧区域重新分布到背侧区域。基于EIT的最佳PEEP在PP时显著低于仰卧位。最佳PEEP的中位数(四分位间距)从14(12 - 16)降至10(8 - 14)cmH₂O。13例(62%)患者在ECMO上进行PP后静态顺应性增加≥3 mL/cmH₂O。与静态顺应性≤3 mL/cmH₂O的患者相比,该亚组患者的体重指数更高、病毒性肺炎更常见、ECMO持续时间更短且基线VT/VT比值更低(P < 0.01)。
尽管基于EIT的基线潮气量分布可能预测ECMO上PP后静态顺应性的改善,但我们的结果支持PP对所有ECMO患者的生理益处,通过改变肺力学并可能减少呼吸机相关性肺损伤(VILI)。现在需要进一步的研究,包括随机对照试验,以证实ECMO期间PP的潜在益处。