Hergenrather Jeffrey Y, Aviram Joshua, Vysotski Yelena, Campisi-Pinto Salvatore, Lewitus Gil M, Meiri David
Faculty of Biology, Technion-Israel Institute of Technology, Haifa, Israel.
Rambam Maimonides Med J. 2020 Jan 30;11(1):e0001. doi: 10.5041/RMMJ.10384.
The aim of this cross-sectional questionnaire-based study was to identify associations between the doses of cannabinoids and terpenes administered, and symptoms of attention deficit hyperactivity disorder (ADHD).
Participants were adult patients licensed for medical cannabis (MC) treatment who also reported a diagnosis of ADHD by a physician. Data on demographics, ADHD, sleep, and anxiety were collected using self-report questionnaires. Data collected on MC treatment included administration route, cultivator, cultivar name, and monthly dose. Comparison statistics were used to evaluate differences in reported parameters between low (20-30 g, n=18) and high (40-70 g, n=35) MC monthly dose and low adult ADHD self-report scale (ASRS, 0-5) score (i.e. ≤3.17 score, n=30) or high ASRS score (i.e. ≥3.18 score, n=29) subgroups.
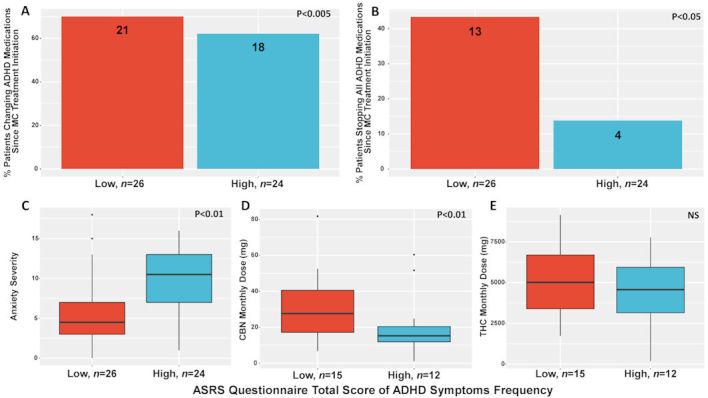
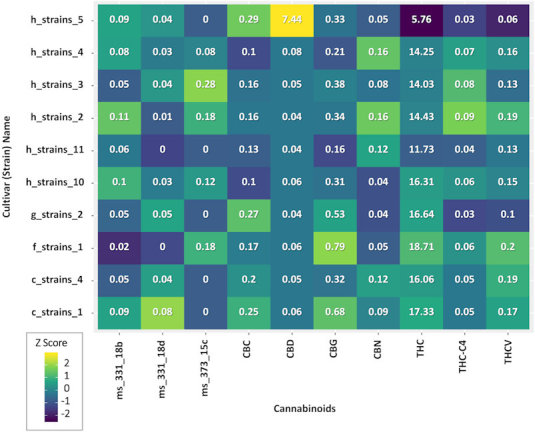
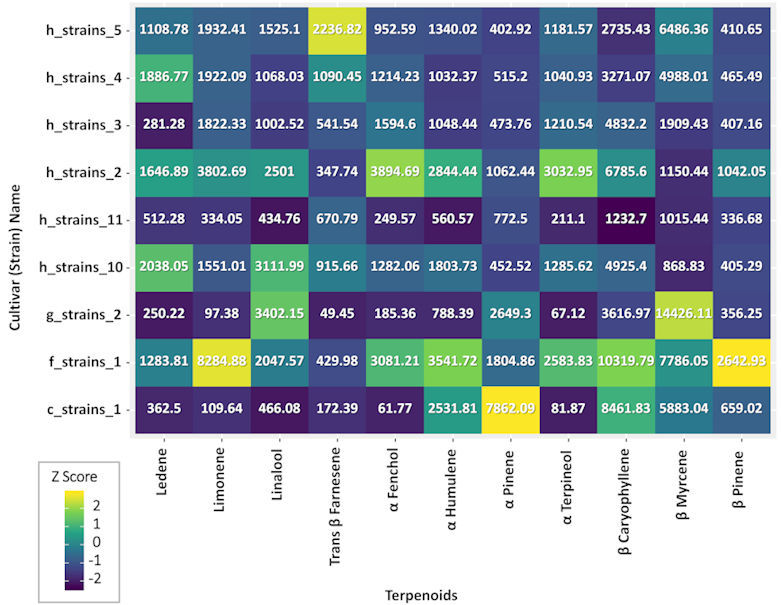
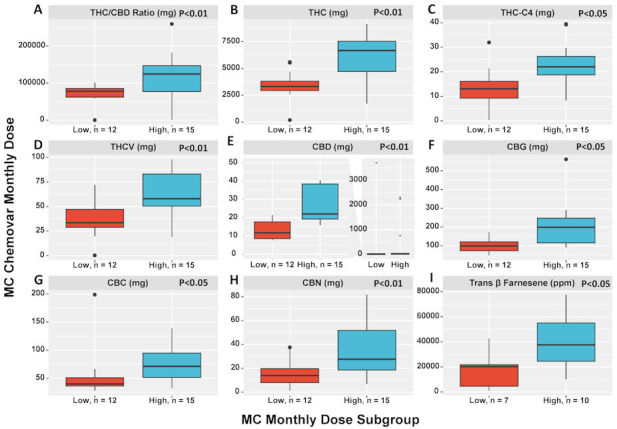
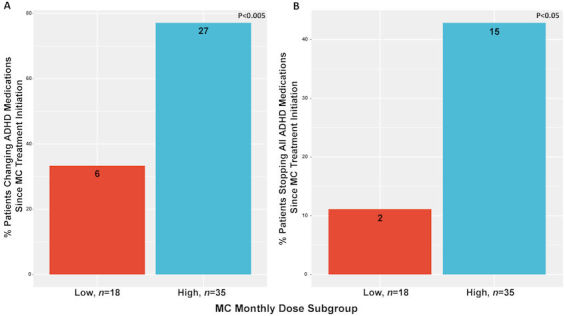
From the 59 patients that answered the questionnaire, MC chemovar could be calculated for 27 (45%) of them. The high MC monthly dose group consumed higher levels of most phyto-cannabinoids and terpenes, but that was not the case for all of the cannabis components. The high dose consumers and the ones with lower ASRS score reported a higher occurrence of stopping all ADHD medications. Moreover, there was an association between lower ASRS score subgroup and lower anxiety scores. In addition, we found an association between lower ASRS score and consumption of high doses of cannabinol (CBN), but not with Δ-9-tetrahydrocannabinol (THC).
These findings reveal that the higher-dose consumption of MC components (phyto-cannabinoids and terpenes) is associated with ADHD medication reduction. In addition, high dosage of CBN was associated with a lower ASRS score. However, more studies are needed in order to fully understand if cannabis and its constituents can be used for management of ADHD.
这项基于问卷调查的横断面研究旨在确定所使用的大麻素和萜烯剂量与注意力缺陷多动障碍(ADHD)症状之间的关联。
参与者为获得医用大麻(MC)治疗许可的成年患者,且有医生诊断其患有ADHD。使用自我报告问卷收集有关人口统计学、ADHD、睡眠和焦虑的数据。收集的关于MC治疗的数据包括给药途径、种植者、品种名称和月剂量。采用比较统计方法评估低(20 - 30克,n = 18)和高(40 - 70克,n = 35)MC月剂量组以及低成人ADHD自我报告量表(ASRS,0 - 5)评分(即≤3.17分,n = 30)或高ASRS评分(即≥3.18分,n = 29)亚组之间报告参数的差异。
在回答问卷的59名患者中,有27名(45%)患者的MC化学型可计算得出。高MC月剂量组摄入的大多数植物大麻素和萜烯水平较高,但并非所有大麻成分都是如此。高剂量使用者和ASRS评分较低者报告停止所有ADHD药物治疗的发生率较高。此外,ASRS评分较低的亚组与较低的焦虑评分之间存在关联。此外,我们发现ASRS评分较低与高剂量大麻酚(CBN)的使用之间存在关联,但与Δ-9-四氢大麻酚(THC)无关。
这些发现表明,较高剂量摄入MC成分(植物大麻素和萜烯)与减少ADHD药物使用有关。此外,高剂量的CBN与较低的ASRS评分有关。然而为了全面了解大麻及其成分是否可用于ADHD的管理,还需要更多的研究。