Liu Fang, Rong Xinxin, Guo Hui, Xu Dong, Liu Chang, Meng Lingling, Yang Xiaoqian, Guo Tingting, Kan Xuefeng, Song Yuhu
Institute of Hematology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China.
Division of Gastroenterology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, China.
BMC Gastroenterol. 2020 Feb 4;20(1):30. doi: 10.1186/s12876-020-1180-0.
One major etiology of hepatic sinusoidal obstruction syndrome (HSOS) in China is the intake of pyrrolizidine alkaloids (PAs). Since PAs-induced HSOS is a rare disease that has not been clearly characterized until now, the aim of this study was to investigate clinical characteristics, CT features, and pathological findings of PA-induced HSOS.
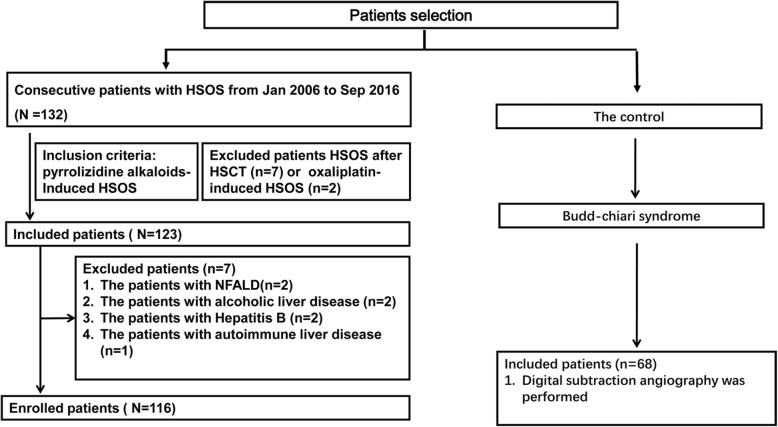
This retrospective cohort study included 116 patients with PAs-induced HSOS and 68 patients with Budd-Chiari syndrome from Jan 2006 to Sep 2016. We collected medical records of the patients, and reviewed image features of CT, and analyzed pathological findings.
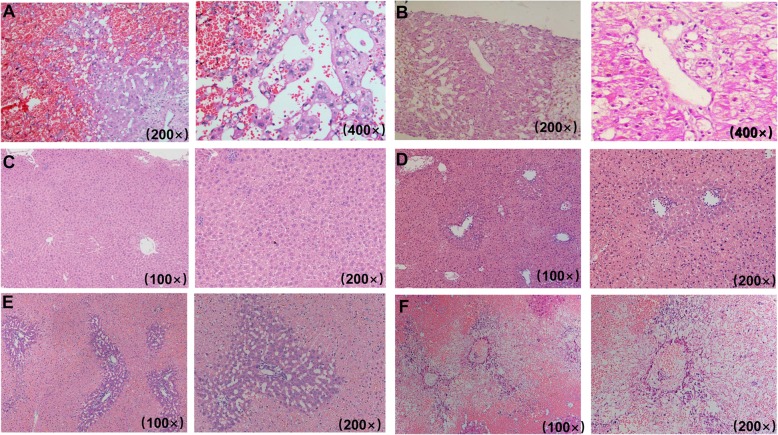
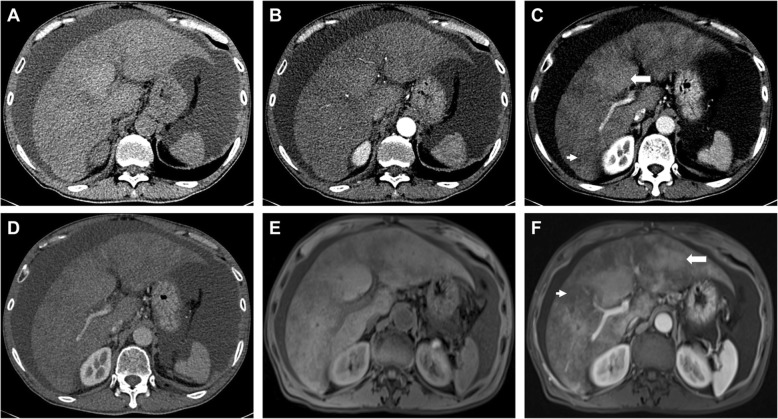
Common clinical manifestations of PAs-induced HSOS were abdominal distention (98.26%), ascites (100%), jaundice (52.94%), abdominal pain (36.36%). Abnormal liver function was observed in most of PAs-induced HSOS. On CT scan, common findings included: ascites, hepatomegaly, the thickening of gallbladder wall, pleural effusion, patchy liver enhancement, and heterogeneous hypoattenuation. Most of the patients had a low ascitic total protein (< 25 g/L) and a high SAAG (≥ 11.0 g/L). In acute stage, pathologic features were massive sinusoidal dilatation, sinusoidal congestion, the extravasation of erythrocytes, hepatocellular necrosis, the accumulation of macrophages, the deposition of hemosiderin. In subacute stage, complete loss of pericentral hepatocytes, sinusoidal dilatation, the deposition of pigment granules were observed.
The PAs-induced HSOS patients displayed distinct clinical characteristics, imaging features, and pathological findings, which provided some evidences for the diagnosis of PAs-induced HSOS.
ChiCTR-DRD-17010709.
在中国,肝窦阻塞综合征(HSOS)的一个主要病因是摄入吡咯里西啶生物碱(PAs)。由于PAs诱导的HSOS是一种罕见疾病,至今尚未得到明确的特征描述,本研究的目的是调查PAs诱导的HSOS的临床特征、CT特征和病理表现。
这项回顾性队列研究纳入了2006年1月至2016年9月期间116例PAs诱导的HSOS患者和68例布加综合征患者。我们收集了患者的病历,回顾了CT图像特征,并分析了病理表现。
PAs诱导的HSOS的常见临床表现为腹胀(98.26%)、腹水(100%)、黄疸(52.94%)、腹痛(36.36%)。大多数PAs诱导的HSOS患者出现肝功能异常。CT扫描常见表现包括:腹水、肝脏肿大、胆囊壁增厚、胸腔积液、肝脏斑片状强化和不均匀低密度。大多数患者腹水总蛋白低(<25 g/L)且血清腹水白蛋白梯度高(≥11.0 g/L)。急性期病理特征为大量肝窦扩张、肝窦充血、红细胞外渗、肝细胞坏死、巨噬细胞积聚、含铁血黄素沉积。亚急性期可见中央周围肝细胞完全丧失、肝窦扩张、色素颗粒沉积。
PAs诱导的HSOS患者表现出独特的临床特征、影像学特征和病理表现,为PAs诱导的HSOS的诊断提供了一些依据。
ChiCTR-DRD-17010709。