Wong Carlos K H, Chen Julie, Fung Samuel K S, Mok Maggie, Cheng Yuk Lun, Kong Irene, Lo Wai Kei, Lui Sing Leung, Chan T M, Lam Cindy L K
Department of Family Medicine and Primary Care, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Rm 1-01, 1/F, Jockey Club Building for Interdisciplinary Research, 5 Sassoon Road, Pokfulam, Hong Kong, China.
Bau Institute of Medical and Health Sciences Education, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong, China.
BMC Nephrol. 2020 Feb 4;21(1):42. doi: 10.1186/s12882-020-1708-0.
This study aimed to determine the lifetime cost-effectiveness of first-line dialysis modalities for end-stage renal disease (ESRD) patients under the "Peritoneal Dialysis First" policy.
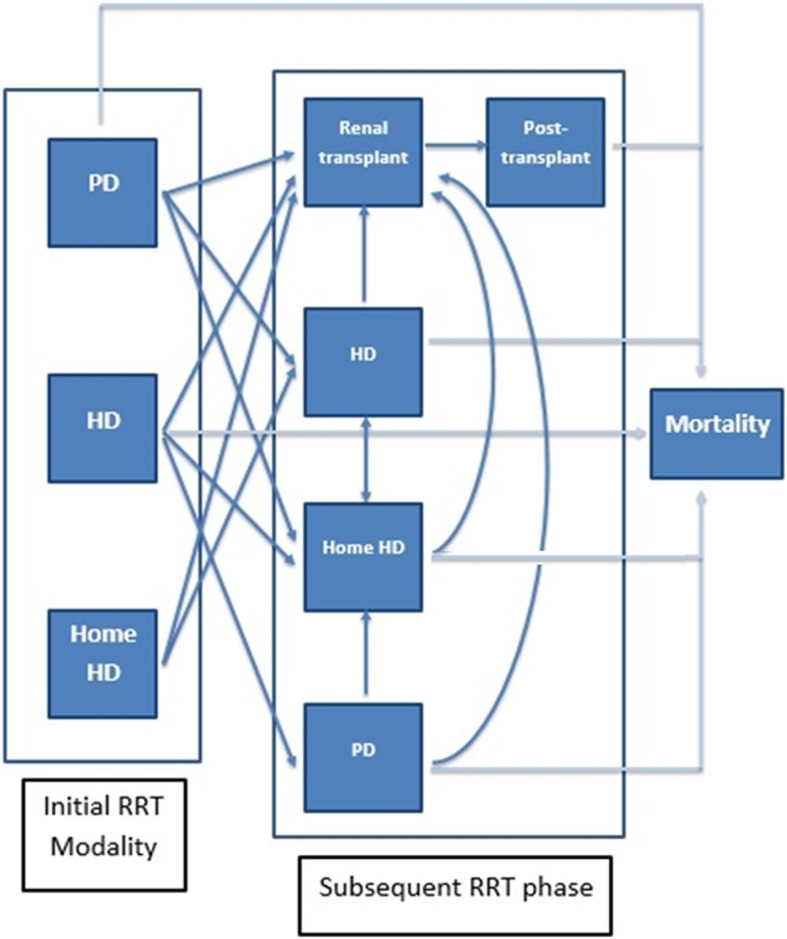
Lifetime cost-effectiveness analyses from both healthcare provider and societal perspectives were performed using Markov modelling by simulating at age 60. Empirical data on costs and health utility scores collected from our studies were combined with published data on health state transitions and survival data to estimate the lifetime cost, quality-adjusted life-years (QALYs) and cost-effectiveness of three competing dialysis modalities: peritoneal dialysis (PD), hospital-based haemodialysis (HD) and nocturnal home HD.
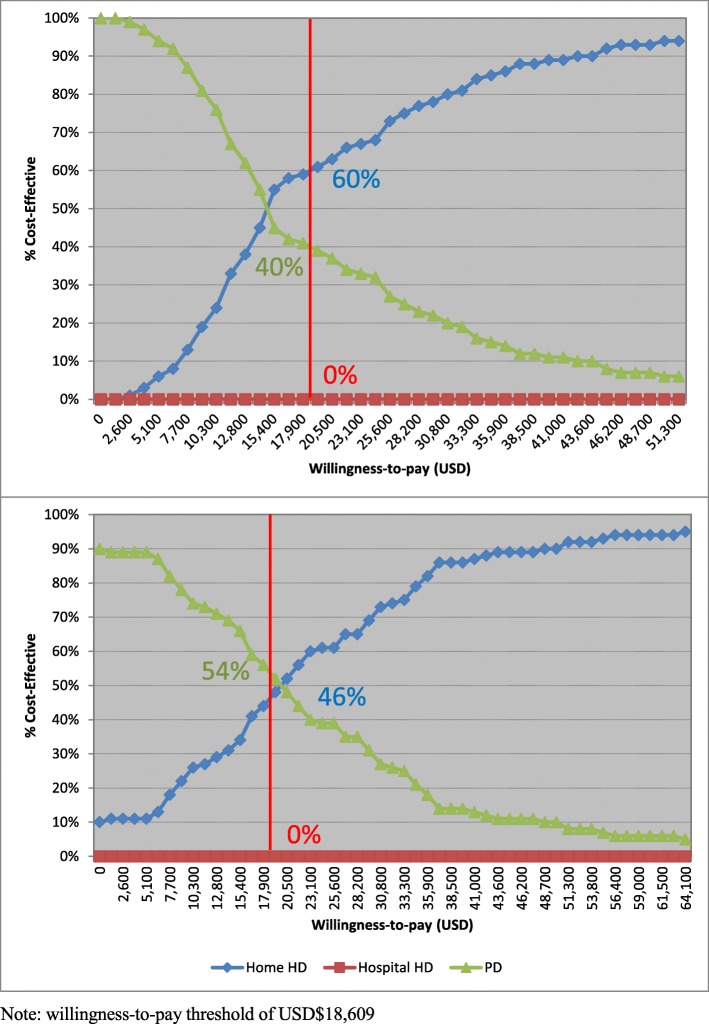
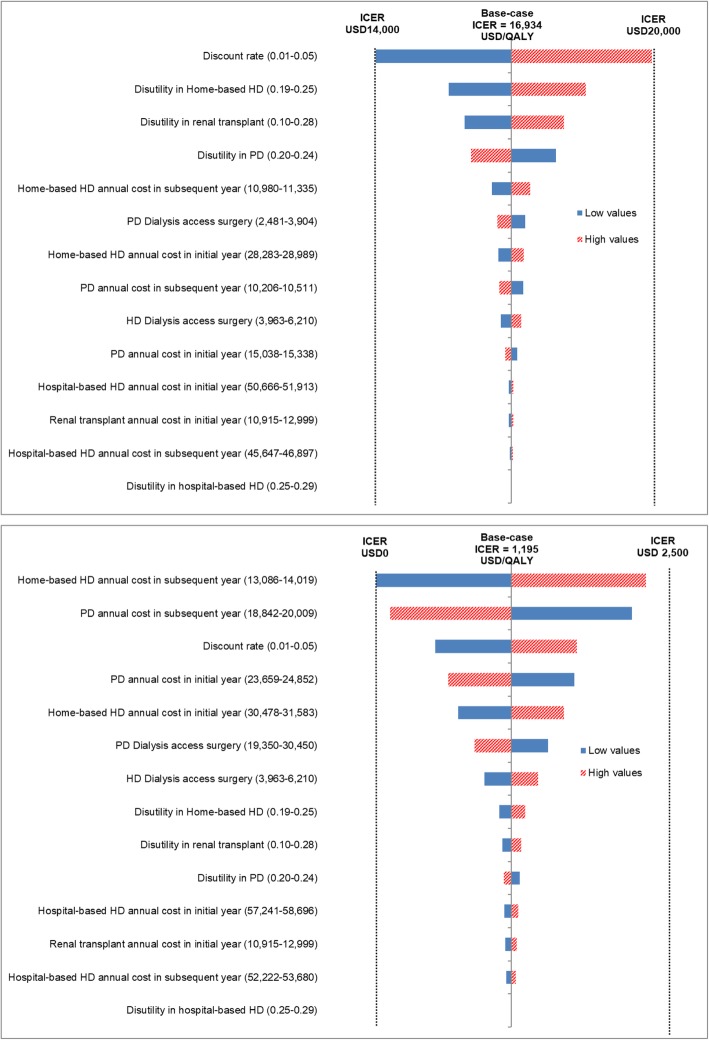
For cost-effectiveness analysis over a lifetime horizon from the perspective of healthcare provider, hospital-based HD group (lifetime cost USD$142,389; 6.58 QALYs) was dominated by the PD group (USD$76,915; 7.13 QALYs). Home-based HD had the highest effectiveness (8.37 QALYs) but with higher cost (USD$97,917) than the PD group. The incremental cost-effectiveness ratio (ICER) was USD$16,934 per QALY gained for home-based HD over PD. From the societal perspective, the results were similar and the ICER was USD$1195 per QALY gained for home-based HD over PD. Both ICERs fell within the acceptable thresholds. Changes in model parameters via sensitivity analyses had a minimal impact on ICER values.
This study assessed the cost-effectiveness of dialysis modalities and service delivery models for ESRD patients under "Peritoneal Dialysis First" policy. For both healthcare provider and societal perspectives, PD as first-line dialysis modality was cost-saving relative to hospital-based HD, supporting the existing PD First or favoured policy. When compared with PD, Nocturnal home Home-based HD was considered a cost-effective first-line dialysis modality for ESRD patients.
本研究旨在确定在“优先选择腹膜透析”政策下,终末期肾病(ESRD)患者一线透析方式的终身成本效益。
采用马尔可夫模型,通过模拟60岁时的情况,从医疗服务提供者和社会角度进行终身成本效益分析。将我们研究中收集的成本和健康效用评分的实证数据与已发表的健康状态转变数据和生存数据相结合,以估计三种竞争性透析方式的终身成本、质量调整生命年(QALYs)和成本效益:腹膜透析(PD)、医院血液透析(HD)和夜间家庭血液透析。
从医疗服务提供者的角度进行终身成本效益分析时,医院血液透析组(终身成本142,389美元;6.58个QALYs)被腹膜透析组(76,915美元;7.13个QALYs)所主导。家庭血液透析的效果最高(8.37个QALYs),但成本(97,917美元)高于腹膜透析组。家庭血液透析相对于腹膜透析每获得一个QALY的增量成本效益比(ICER)为16,934美元。从社会角度来看,结果相似,家庭血液透析相对于腹膜透析每获得一个QALY的ICER为1195美元。两个ICER均落在可接受的阈值范围内。通过敏感性分析对模型参数进行的更改对ICER值的影响最小。
本研究评估了“优先选择腹膜透析”政策下ESRD患者透析方式和服务提供模式的成本效益。从医疗服务提供者和社会角度来看,作为一线透析方式的腹膜透析相对于医院血液透析具有成本节约优势,支持现有的优先选择腹膜透析或优惠政策。与腹膜透析相比,夜间家庭血液透析被认为是ESRD患者具有成本效益的一线透析方式。