Department of Diagnostic and Interventional Radiology, Lausanne University Hospital and University of Lausanne, Rue du Bugnon 46, 1011, Lausanne, Switzerland.
Department of Radiology, Riviera-Chablais Hospital, Avenue de la Prairie 10, 1800, Vevey, Switzerland.
Eur Radiol. 2020 May;30(5):2583-2593. doi: 10.1007/s00330-019-06626-6. Epub 2020 Feb 4.
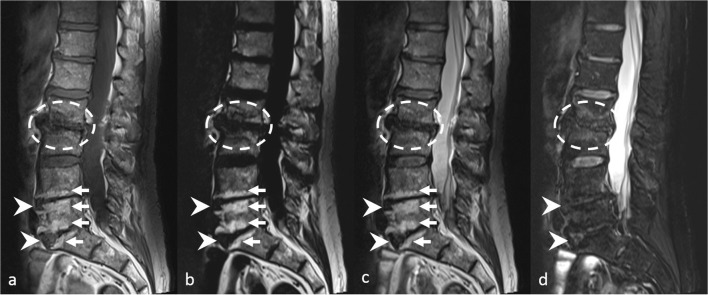
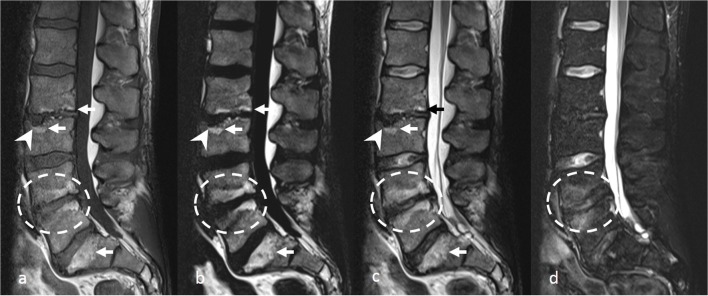
To show that for the MRI workup of non-specific low back pain and/or lumbar radiculopathy, the acquisition of T1-weighted sequences in the sagittal plane could be waived when using an FSE T2-weighted Dixon sequence.
Three musculoskeletal radiologists retrospectively reviewed fifty lumbar spine MRI examinations performed for non-specific low back pain and/or lumbar radiculopathy. Two protocols were separately analyzed in the sagittal plane: a standard protocol (T1-weighted, in-phase, and water-only images of an FSE T2-weighted Dixon sequence) and a simplified protocol (fat-only, in-phase, and water-only images of an FSE T2-weighted Dixon sequence). Eight items usually assessed on T1-weighted sequences were analyzed for each of the vertebrae (n = 250), vertebral endplates (n = 500), vertebral corners (n = 1000), foramina (n = 500), lamina (n = 500), and facet joints (n = 500). Interchangeability of these protocols was tested using the individual equivalence index. A decrease in interobserver agreement of ≥ 5% when one reader used the simplified protocol compared with when both readers used the standard protocol was considered clinically significant. Interreader and intrareader agreement were assessed using kappa statistics. Rates of findings with each protocol were compared using odd ratios.
The standard and simplified protocols were interchangeable (range of upper bound of the 95%CI of individual equivalence index = 0.25 to 1.38%). Intraprotocol and interprotocol interreader kappa values were similar (0.253-0.671 vs. 0.236-0.723, respectively). Rates of findings were not statistically significantly different (p ≥ 0.074), or were higher with the simplified protocol (p ≤ 0.036).
In our target population, a single sagittal T2-weighted Dixon sequence may replace the recommended combination of T1-, T2-, and fat-suppressed T2-weighted sequences.
• In patients with non-specific low back pain or lumbar radiculopathy, spine MRI in the sagittal plane could be limited to a single FSE T2-weighted Dixon sequence, hereby reducing the acquisition time. • A simplified protocol of spine MRI in the sagittal plane combining FSE T2-weighted Dixon sequence provides the same information as a standard protocol including T1-, T2-, and fat-suppressed T2-weighted sequences for the workup of degenerative lumbar spine lesions. • For some findings shown on the simplified protocol, such as focal bone marrow replacement lesions or signs of infection, additional sequences including pre- and post-contrast T1-weighted sequences may be required, as is currently the case when using the standard protocol.
展示在非特异性下腰痛和/或腰椎神经根病的 MRI 检查中,当使用 FSE T2 加权 Dixon 序列时,可以放弃矢状面 T1 加权序列的采集。
三位肌肉骨骼放射科医生回顾性分析了 50 例因非特异性下腰痛和/或腰椎神经根病而行腰椎 MRI 检查的患者。分别在矢状面分析两种方案:标准方案(FSE T2 加权 Dixon 序列的 T1 加权、同相位、仅含水像)和简化方案(FSE T2 加权 Dixon 序列的仅含脂肪、同相位、仅含水像)。分析了每个椎体(n=250)、椎体终板(n=500)、椎体角(n=1000)、椎间孔(n=500)、椎板(n=500)和关节突关节(n=500)的 8 个项目。使用个体等效指数测试这些方案的可互换性。当一位读者使用简化方案时,如果与两位读者都使用标准方案相比,观察者间一致性降低≥5%,则认为具有临床意义。使用 Kappa 统计评估观察者内和观察者间的一致性。使用比值比比较每个方案的检出率。
标准和简化方案是可互换的(个体等效指数上限的 95%CI 范围为 0.25 至 1.38%)。同方案和异方案的观察者间 Kappa 值相似(分别为 0.253-0.671 和 0.236-0.723)。检出率无统计学差异(p≥0.074),或简化方案更高(p≤0.036)。
在我们的目标人群中,单个矢状面 T2 加权 Dixon 序列可能取代推荐的 T1、T2 和脂肪抑制 T2 加权序列的组合。
在患有非特异性下腰痛或腰椎神经根病的患者中,脊柱 MRI 矢状面检查可仅限于单个 FSE T2 加权 Dixon 序列,从而减少采集时间。
简化的脊柱 MRI 矢状面方案结合 FSE T2 加权 Dixon 序列,可提供与标准方案相同的信息,包括 T1、T2 和脂肪抑制 T2 加权序列,用于退行性腰椎病变的评估。
对于简化方案中显示的一些发现,例如局灶性骨髓替代病变或感染迹象,可能需要包括对比前和对比后的 T1 加权序列等其他序列,这与当前使用标准方案的情况相同。