Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom.
National Cancer Registration and Analysis Service, Public Health England, London, United Kingdom.
Int J Cancer. 2020 Sep 1;147(5):1437-1449. doi: 10.1002/ijc.32908. Epub 2020 Mar 4.
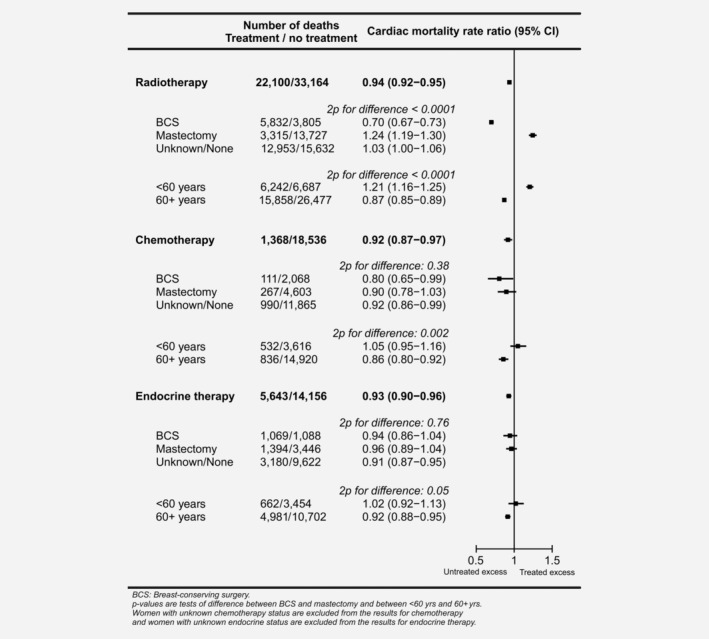
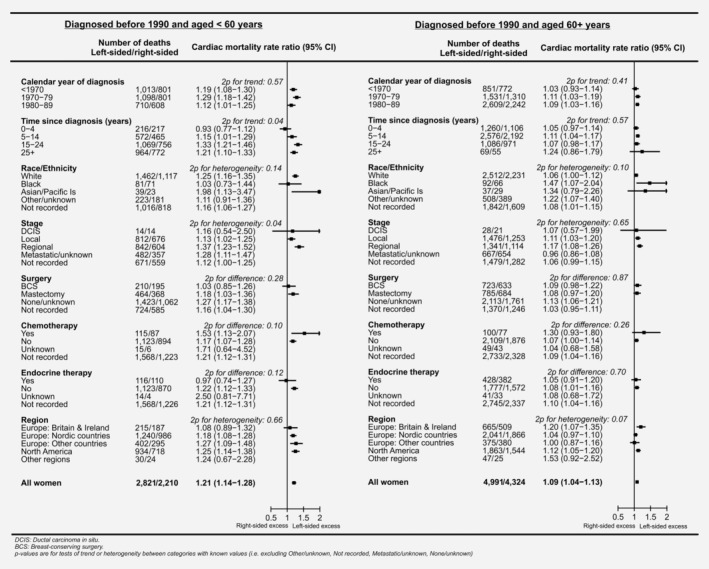
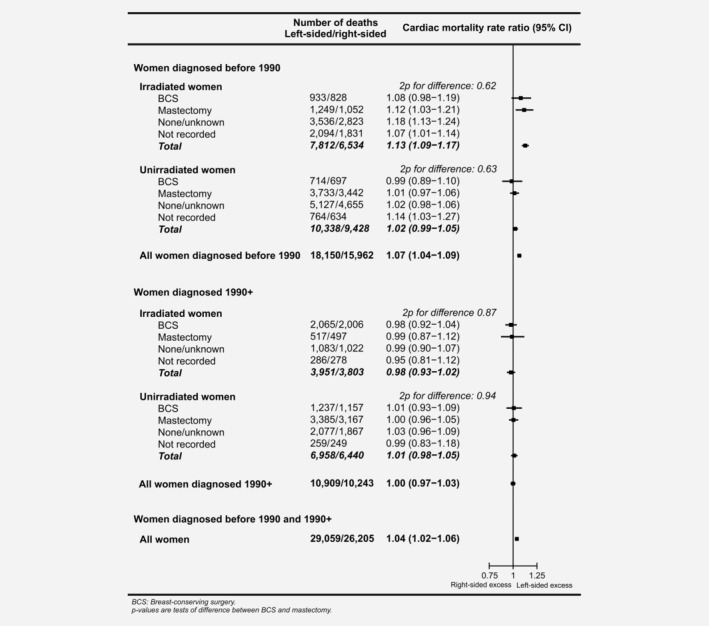
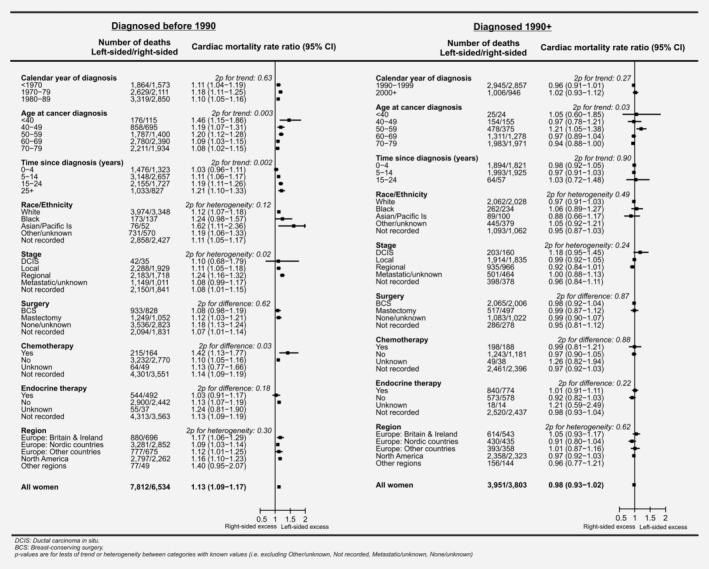
Comparisons of patients receiving different cancer treatments reflect the effects of both treatment and patient selection. In breast cancer, however, if radiotherapy decisions are unrelated to laterality, comparisons of left-sided and right-sided cancers can demonstrate the causal effects of higher-versus-lower cardiac radiation dose. Cardiac mortality was analysed using individual patient data for 1,934,248 women with breast cancer in 22 countries. The median date of diagnosis was 1996 and the interquartile range was 1987-2002. A total of 1,018,505 women were recorded as irradiated, 223,077 as receiving chemotherapy, 317,619 as receiving endocrine therapy and 55,264 died of cardiac disease. Analyses were stratified by time since breast cancer diagnosis, age at diagnosis, calendar year of diagnosis and country. Patient-selection effects were evident for all three treatments. For radiotherapy, there was also evidence of selection according to laterality in women irradiated 1990 or later. In patients irradiated before 1990, there was no such selection and cardiac mortality was higher in left-sided than right-sided cancer (rate ratio [RR]: 1.13, 95% confidence interval 1.09-1.17). Left-versus-right cardiac mortality RRs were greater among younger women (1.46, 1.19, 1.20, 1.09 and 1.08 after cancer diagnoses at ages <40, 40-49, 50-59, 60-69 and 70+ years, 2p =0.003). Left-versus-right RRs also increased with time since cancer diagnosis (1.03, 1.11, 1.19 and 1.21 during 0-4, 5-14, 15-24 and 25+ years, 2p =0.002) while for women who also received chemotherapy, the left-versus-right RR was 1.42 (95% confidence interval 1.13-1.77), compared to 1.10 (1.05-1.16) for women who did not (2p = 0.03). These results show that the relative increase in cardiac mortality from cardiac exposure during breast cancer radiotherapy given in the past was greater in younger women, lasted into the third decade after exposure and was greater when chemotherapy was also given.
不同癌症治疗方法的患者比较反映了治疗和患者选择的综合影响。然而,在乳腺癌中,如果放疗决策与侧别无关,那么对左侧和右侧乳腺癌的比较可以证明较高与较低心脏辐射剂量的因果效应。对 22 个国家的 1934248 名乳腺癌患者的个体患者数据进行了心脏死亡率分析。中位诊断日期为 1996 年,四分位距为 1987-2002 年。共有 1018505 名妇女被记录为接受了放疗,223077 名妇女接受了化疗,317619 名妇女接受了内分泌治疗,55264 名妇女死于心脏病。分析按乳腺癌诊断后时间、诊断时年龄、诊断年份和国家进行分层。所有三种治疗方法均存在明显的患者选择效应。对于放疗,在 1990 年或以后接受放疗的妇女中,也存在根据侧别进行选择的证据。在 1990 年前接受放疗的患者中,没有这种选择,左侧乳腺癌的心脏死亡率高于右侧(比率比 [RR]:1.13,95%置信区间 1.09-1.17)。年轻女性的左-右心脏死亡率 RR 更高(<40 岁、40-49 岁、50-59 岁、60-69 岁和 70 岁及以上的癌症诊断后分别为 1.46、1.19、1.20、1.09 和 1.08,2p =0.003)。左-右 RR 也随癌症诊断后时间而增加(0-4 年、5-14 年、15-24 年和 25+年分别为 1.03、1.11、1.19 和 1.21,2p =0.002),而对于同时接受化疗的女性,左-右 RR 为 1.42(95%置信区间 1.13-1.77),而未接受化疗的女性为 1.10(1.05-1.16)(2p = 0.03)。这些结果表明,过去接受乳腺癌放疗时心脏暴露导致的心脏死亡率相对增加在年轻女性中更大,持续到暴露后的第三个十年,并且当同时给予化疗时更大。