Luo Ma, Chen Si-Liang, Chen Jiawen, Yan Huzheng, Qiu Zhenkang, Chen Guanyu, Lu Ligong, Zhang Fujun
Sun Yat-sen University Cancer Center; State Key Laboratory of Oncology in South China; Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Zhuhai Interventional Medical Center, Zhuhai Precision Medical Center, Zhuhai People's Hospital, Zhuhai Hospital Affiliated with Jinan University, Zhuhai, Guangdong, China.
PeerJ. 2020 Jan 27;8:e8398. doi: 10.7717/peerj.8398. eCollection 2020.
There has been no prospective or retrospective studies reporting the comparison outcome between surgery and ablation for resectable-ablative (lesions could be treated by resection or complete ablation) colorectal liver oligometastases (CLOM). The purpose of this study was to compare the efficacy and prognostic difference in patients who underwent R0 resection vs. complete ablation within the resectable-ablative CLOM criteria.
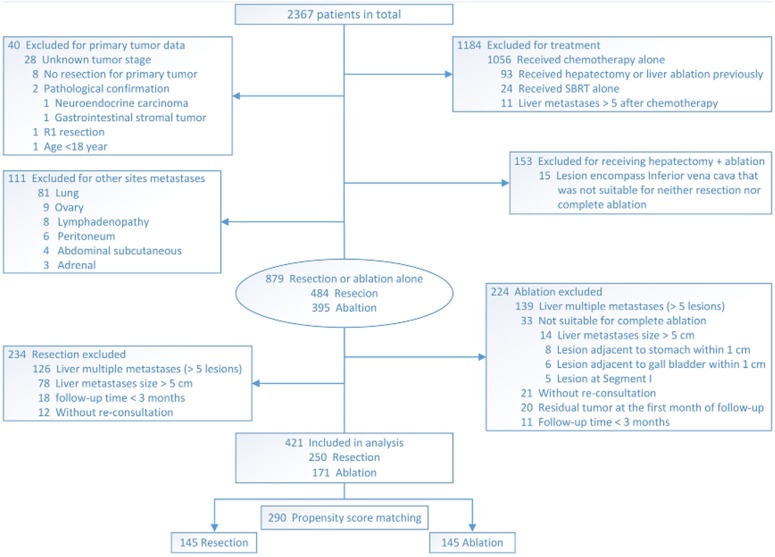
From January 2008 to May 2018, a total of 2,367 patients diagnosed with colorectal liver metastases were included in this observational study. The metastasis was characterized by only limited to liver with number ≤5, size ≤5 cm, and resectable-ablative (lesions could be treated by resection or complete ablation). The evaluated indications, including liver progression-free survival (LPFS), overall survival (OS), survival rates, pattern and number of recurrences, and complications, were compared by using propensity score matching (PSM). The Kaplan-Meier curves were generated, and a log-rank test was performed. The Cox regression model was used for univariate and multivariate analyses to identify predictors of outcomes.
A total of 421 consecutive patients were eligible for this study, with 250 and 171 undergoing R0 resection and complete ablation, respectively. PSM identified 145 patients from each group. The 1-, 3-, 5- and 8-year OS rates in the resection group and the ablation group were 95.8% vs. 95.0%, 69.8% vs. 60.1%, 53.6% vs. 42.5%, and 45.1% vs. 32.9% ( = 0.075), respectively. The median LPFS in the resection group was significantly longer than that in the ablation group (35 months vs. 15 months, = 0.011). No statistical difference was found in LPFS between the two groups when comparing ≤3 cm liver metastases. For liver metastasis >3 cm, the median LPFS in the resection group and ablation group was 11 months and 5 months, respectively ( = 0.001). In terms of high risk of clinical risk score (CRS), the resection group showed longer LPFS than the ablation group (median 18 months vs. 10 months, = 0.043).
For patients within the CLOM criteria suggesting that liver metastases were resectable as well as ablative, resection could result in longer liver recurrence-free survival than ablation in cases with size >3 cm or high risk of CRS. But for ≤3 cm liver metastases, their treatment efficacies were comparable.
目前尚无前瞻性或回顾性研究报告可切除性消融(病灶可通过切除或完全消融治疗)的结直肠癌肝寡转移(CLOM)患者手术与消融治疗的比较结果。本研究的目的是比较符合可切除性消融CLOM标准的患者接受R0切除与完全消融后的疗效及预后差异。
2008年1月至2018年5月,本观察性研究共纳入2367例诊断为结直肠癌肝转移的患者。转移灶的特征为仅局限于肝脏,数量≤5个,大小≤5 cm,且为可切除性消融(病灶可通过切除或完全消融治疗)。通过倾向评分匹配(PSM)比较评估指标,包括无肝进展生存期(LPFS)、总生存期(OS)、生存率、复发模式和数量以及并发症。绘制Kaplan-Meier曲线,并进行对数秩检验。采用Cox回归模型进行单因素和多因素分析,以确定预后的预测因素。
共有421例连续患者符合本研究条件,其中250例和171例分别接受了R0切除和完全消融。PSM在每组中各确定了145例患者。切除组和消融组的1年、3年、5年和8年总生存率分别为95.8%对95.0%、69.8%对60.1%、53.6%对42.5%、45.1%对32.9%(P = 0.075)。切除组的中位LPFS显著长于消融组(35个月对15个月,P = 0.011)。比较≤3 cm肝转移灶时,两组的LPFS无统计学差异。对于>3 cm的肝转移灶,切除组和消融组的中位LPFS分别为11个月和5个月(P = 0.001)。在临床风险评分(CRS)高危方面,切除组的LPFS长于消融组(中位18个月对10个月,P = 0.043)。
对于符合CLOM标准提示肝转移灶可切除且可消融的患者,在转移灶大小>3 cm或CRS高危的情况下,手术切除可导致比消融更长的无肝复发生存期。但对于≤3 cm的肝转移灶,两者的治疗效果相当。