Experimental and Clinical Pharmacology, Department of Medical Biology, UiT, The Arctic University of Norway, 9037 Tromsø, Norway.
Anesthesia and Critical Care Research Group, Department of Clinical Medicine, UiT, The Arctic University of Norway, Norway.
Cardiovasc Res. 2020 Nov 1;116(13):2081-2090. doi: 10.1093/cvr/cvz309.
Treatment of arrhythmias evoked by hypothermia/rewarming remains challenging, and the underlying mechanisms are unclear. This in vitro experimental study assessed cardiac electrophysiology in isolated rabbit hearts at temperatures occurring in therapeutic and accidental hypothermia.
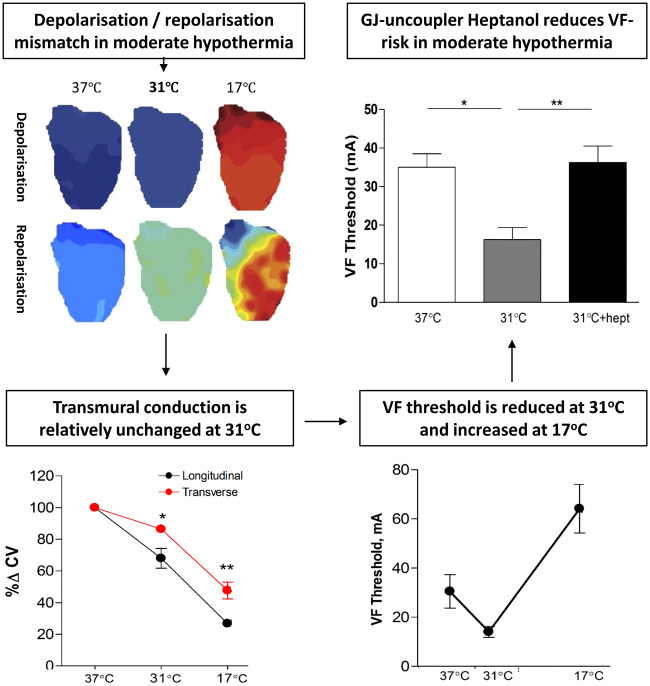
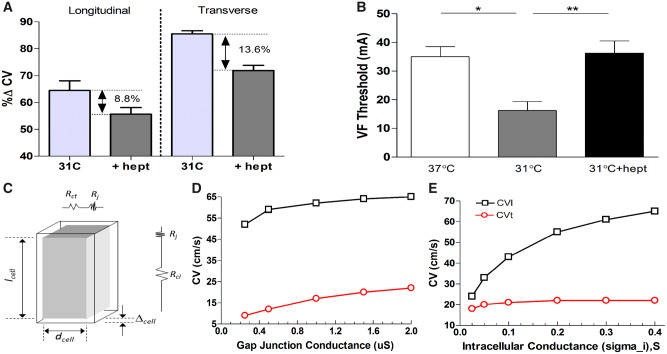
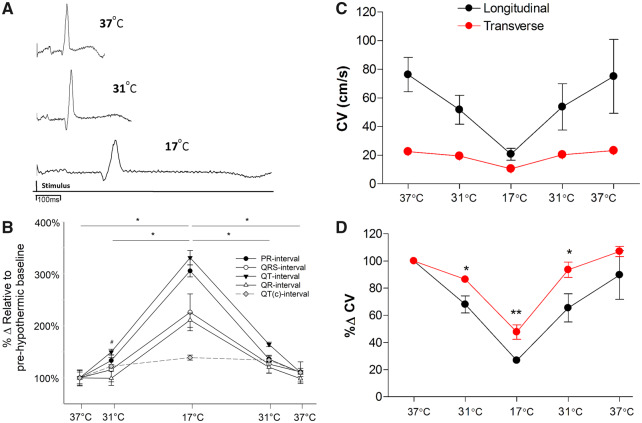
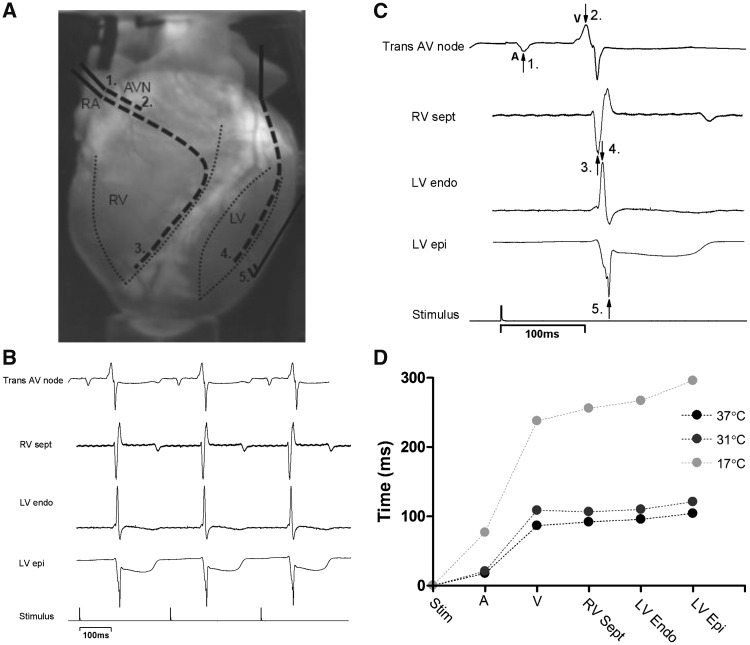
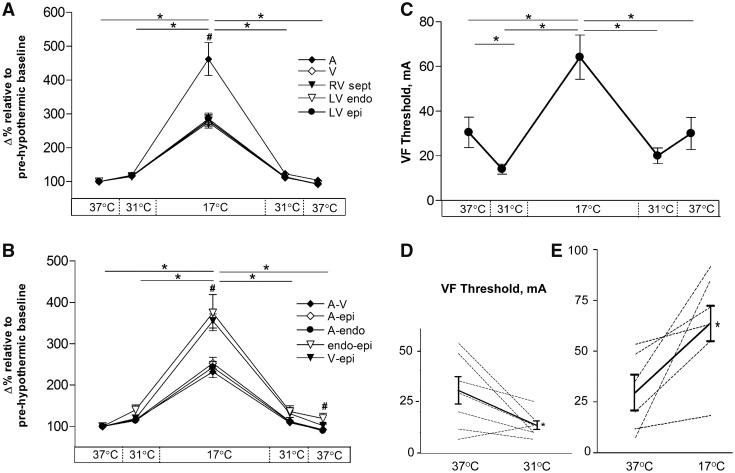
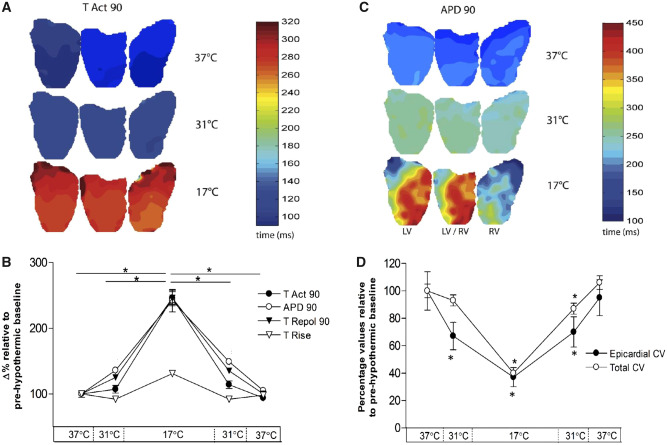
Detailed ECG, surface electrogram, and panoramic optical mapping were performed in isolated rabbit hearts cooled to moderate (31°C) and severe (17°C) hypothermia. Ventricular activation was unchanged at 31°C while action potential duration (APD) was significantly prolonged (176.9 ± 4.2 ms vs. 241.0 ± 2.9 ms, P < 0.05), as was ventricular repolarization. At 17°C, there were proportionally similar delays in both activation and repolarization. These changes were reflected in the QRS and QT intervals of ECG recordings. Ventricular fibrillation threshold was significantly reduced at 31°C (16.3 ± 3.1 vs. 35 ± 3.5 mA, P < 0.05) but increased at 17°C (64.2 ± 9.9, P < 0.05). At 31°C, transverse conduction was relatively unchanged by cooling compared to longitudinal conduction, but at 17°C both transverse and longitudinal conduction were proportionately reduced to a similar extent. The gap junction uncoupler heptanol had a larger relative effect on transverse than longitudinal conduction and was able to restore the transverse/longitudinal conduction ratio, returning ventricular fibrillation threshold to baseline values (16.3 ± 3.1 vs. 36.3 ± 4.3 mA, P < 0.05) at 31°C. Rewarming to 37°C restored the majority of the electrophysiological parameters.
Moderate hypothermia does not significantly change ventricular conduction time but prolongs repolarization and is pro-arrhythmic. Further cooling to severe hypothermia causes parallel changes in ventricular activation and repolarization, changes which are anti-arrhythmic. Therefore, relative changes in QRS and QT intervals (QR/QTc) emerge as an ECG-biomarker of pro-arrhythmic activity. Risk for ventricular fibrillation appears to be linked to the relatively low temperature sensitivity of ventricular transmural conduction, a conclusion supported by the anti-arrhythmic effect of heptanol at 31°C.
低温/复温诱发的心律失常的治疗仍然具有挑战性,其潜在机制尚不清楚。这项离体实验研究评估了在治疗和意外低温中发生的温度下,分离兔心的心脏电生理学。
在冷却至中度(31°C)和重度(17°C)低温的分离兔心中进行详细的心电图、表面电图和全景光学映射。在 31°C 时心室激活没有改变,而动作电位持续时间(APD)显著延长(176.9±4.2 ms 比 241.0±2.9 ms,P<0.05),心室复极也是如此。在 17°C 时,激活和复极的延迟比例相似。这些变化反映在心电图记录的 QRS 和 QT 间隔中。在 31°C 时,心室颤动阈值显著降低(16.3±3.1 比 35±3.5 mA,P<0.05),但在 17°C 时增加(64.2±9.9,P<0.05)。在 31°C 时,与纵向传导相比,冷却对横向传导的影响相对较小,但在 17°C 时,横向和纵向传导都按比例减少到相似程度。缝隙连接解偶联剂庚醇对横向传导的相对影响大于纵向传导,并且能够恢复横向/纵向传导比,使心室颤动阈值恢复到基线值(16.3±3.1 比 36.3±4.3 mA,P<0.05)在 31°C 时。复温至 37°C 可恢复大多数电生理参数。
中度低温不会显著改变心室传导时间,但会延长复极并引起心律失常。进一步冷却至严重低温会导致心室激活和复极的平行变化,这些变化具有抗心律失常作用。因此,QRS 和 QT 间隔(QR/QTc)的相对变化成为心律失常活动的心电图生物标志物。心室颤动的风险似乎与心室透壁传导的相对低温敏感性有关,庚醇在 31°C 时的抗心律失常作用支持了这一结论。