Department of Medical and Surgical Sciences, University Magna Græcia of Catanzaro, 88100 Catanzaro, Italy.
Internal Medicine Unit, Pugliese-Ciaccio Hospital, 88100 Catanzaro, Italy.
Nutrients. 2020 Feb 5;12(2):412. doi: 10.3390/nu12020412.
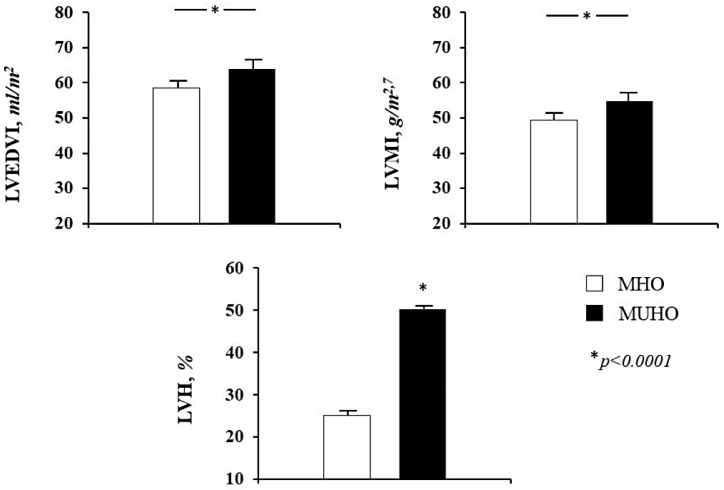
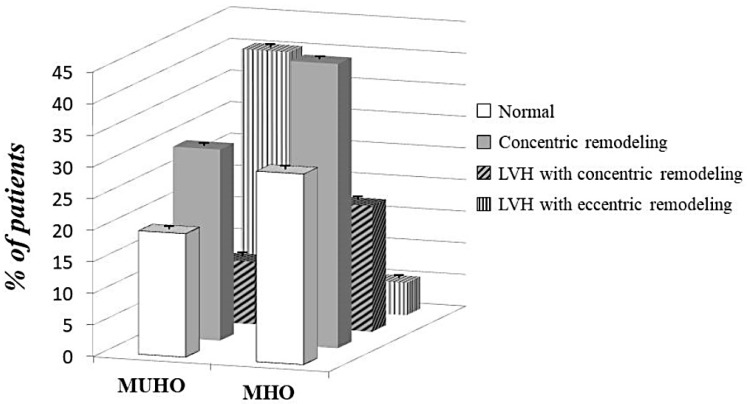
Obese subjects showed different cardiovascular risk depending by different insulin sensitivity status. We investigated the difference in left ventricular mass and geometry between metabolically healthy (MHO) and unhealthy (MUHO) obese subjects. From a cohort of 876 obese subjects (48.3 ± 14.1 years) without cardio-metabolic disease and stratified according to increasing values of Matsuda index after 75 g oral glucose tolerance test, we defined MHO ( = 292) those in the upper tertile and MUHO ( = 292) those in the lower tertile. All participants underwent echocardiographic measurements. Left ventricular mass was calculated by Devereux equation and normalized by height and left ventricular hypertrophy (LVH) was defined by values >44 g/m for females and >48 g/m for males. Left ventricular geometric pattern was defined as concentric or eccentric if relative wall thickness was higher or lower than 0.42, respectively. MHO developed more commonly a concentric remodeling (19.9 vs. 9.9%; = 0.001) and had a reduced risk for LVH (OR 0.46; < 0.0001) than MUHO, in which the eccentric type was more prevalent (40.4 vs. 5.1%; < 0.0001). We demonstrated that obese subjects-matched for age, gender and BMI-have different left ventricular mass and geometry due to different insulin sensitivity status, suggesting that diverse metabolic phenotypes lead to alternative myocardial adaptation.
肥胖患者的心血管风险因胰岛素敏感性状态的不同而不同。我们研究了代谢健康(MHO)和代谢不健康(MUHO)肥胖患者之间左心室质量和几何形状的差异。从 876 名无心脏代谢疾病的肥胖患者队列(48.3 ± 14.1 岁)中,根据 75g 口服葡萄糖耐量试验后 Matsuda 指数的增加值进行分层,我们将上三分之一定义为代谢健康(MHO,= 292),下三分之一定义为代谢不健康(MUHO,= 292)。所有参与者均接受了超声心动图检查。左心室质量通过 Devereux 方程计算,并按身高和左心室质量指数进行归一化,左心室肥厚(LVH)定义为女性>44g/m 和男性>48g/m。左心室几何形状如果相对室壁厚度高于或低于 0.42,则定义为向心性或偏心性。MHO 更常见同心重构(19.9%比 9.9%;= 0.001),并且发生 LVH 的风险降低(OR 0.46;<0.0001),而 MUHO 中更常见偏心型(40.4%比 5.1%;<0.0001)。我们证明了年龄、性别和 BMI 匹配的肥胖患者,由于胰岛素敏感性状态的不同,左心室质量和几何形状存在差异,这表明不同的代谢表型导致了不同的心肌适应性。