Jo Taisuke, Yasunaga Hideo, Yamauchi Yasuhiro, Mitani Akihisa, Hiraishi Yoshihisa, Hasegawa Wakae, Sakamoto Yukiyo, Matsui Hiroki, Fushimi Kiyohide, Nagase Takahide
Dept of Health Services Research, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
Dept of Respiratory Medicine, Graduate School of Medicine, The University of Tokyo, Tokyo, Japan.
ERJ Open Res. 2020 Feb 3;6(1). doi: 10.1183/23120541.00246-2019. eCollection 2020 Jan.
Inhaled corticosteroids (ICSs) are used for advanced-stage chronic obstructive pulmonary disease (COPD). The application and safety of ICS withdrawal remain controversial.This study aimed to evaluate the association between ICS withdrawal and outcomes in elderly patients with COPD with or without comorbid bronchial asthma, who were hospitalised for exacerbation.
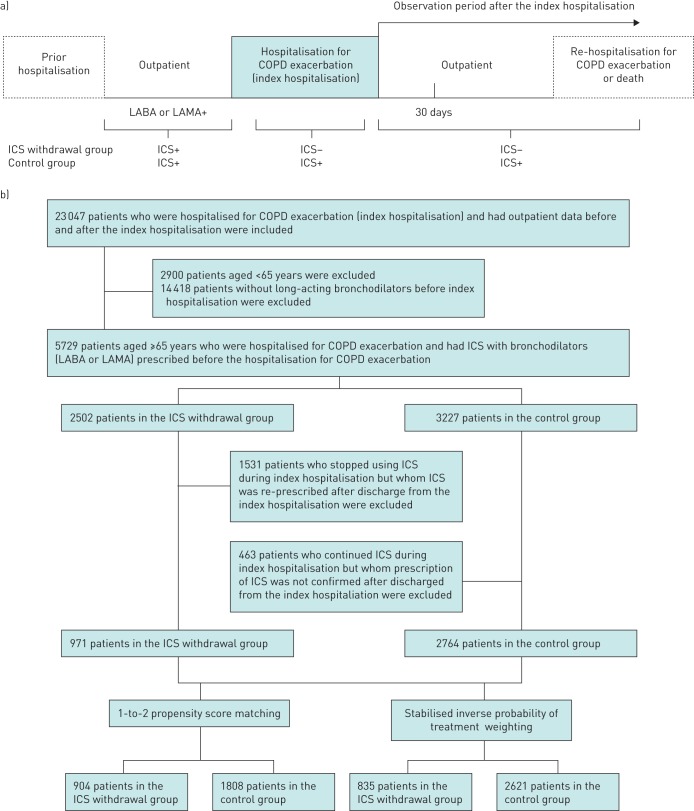
We conducted a retrospective cohort study using the Japanese Diagnosis Procedure Combination database from July 2010 to March 2016 We identified patients aged ≥65 years who were hospitalised for COPD exacerbation. Re-hospitalisation for COPD exacerbation or death, frequency of antimicrobial medicine prescriptions and frequency of oral corticosteroid prescriptions after discharge were compared between patients with withdrawal and continuation of ICSs using propensity score analyses, namely 1-2 propensity score matching and stabilised inverse probability of treatment weighting.
Among 3735 eligible patients, 971 and 2764 patients had ICS withdrawal and continuation, respectively. The hazard ratios (95% confidence intervals) of re-hospitalisation for COPD exacerbation or death for ICS withdrawal compared to continuation were 0.65 (0.52-0.80) in the propensity score matching and 0.71 (0.56-0.90) in the inverse probability of treatment weighting. The frequency of antimicrobial prescriptions but not corticosteroid prescriptions within 1 year was significantly less in the ICS withdrawal group. Among patients with comorbid bronchial asthma, ICS withdrawal was significantly associated with reduced re-hospitalisation for COPD exacerbation or death only in the propensity score matching analysis.
ICS withdrawal after COPD exacerbation was significantly associated with reduced incidences of re-hospitalisation or death among elderly patients, including those with comorbid bronchial asthma.
吸入性糖皮质激素(ICSs)用于晚期慢性阻塞性肺疾病(COPD)。ICS撤药的应用及安全性仍存在争议。本研究旨在评估因病情加重住院的、患有或未患有合并支气管哮喘的老年COPD患者中,ICS撤药与预后之间的关联。
我们使用日本诊断程序组合数据库进行了一项回顾性队列研究,时间跨度为2010年7月至2016年3月。我们确定了年龄≥65岁、因COPD加重住院的患者。使用倾向评分分析,即1-2倾向评分匹配和稳定的逆概率治疗加权法,比较了ICS撤药组和继续使用ICS组患者因COPD加重再次住院或死亡的情况、出院后抗菌药物处方频率以及口服糖皮质激素处方频率。
在3735例符合条件的患者中,分别有971例和2764例患者停用和继续使用ICS。倾向评分匹配中,与继续使用ICS相比,ICS撤药组因COPD加重再次住院或死亡的风险比(95%置信区间)为0.65(0.52-0.80),逆概率治疗加权法中为0.71(0.56-0.90)。ICS撤药组1年内抗菌药物处方频率显著降低,但糖皮质激素处方频率无显著差异。在合并支气管哮喘的患者中,仅在倾向评分匹配分析中,ICS撤药与因COPD加重再次住院或死亡风险降低显著相关。
COPD加重后停用ICS与老年患者(包括合并支气管哮喘的患者)再次住院或死亡发生率降低显著相关。