Agarwal Aakash, Aker Loai, Ahmad Alaaeldin Azmi
Department of Bioengineering and Orthopaedics Surgery, University of Toledo, Toledo, USA.
Department of Orthopedics, Annajah Medical School, Nablus, West Bank.
Spine Surg Relat Res. 2019 Aug 16;4(1):31-36. doi: 10.22603/ssrr.2019-0045. eCollection 2020.
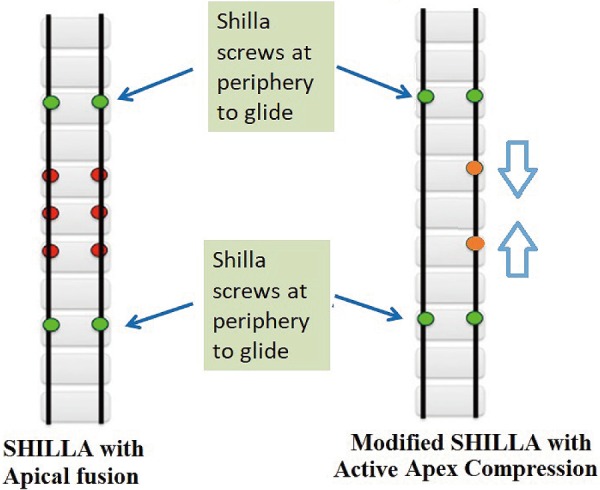
SHILLA and growth rods are two main surgical correction techniques for patients with early-onset scoliosis. There have been some comparative studies between the two techniques, where a comparison was made between deformity identifying characteristics such as Cobb angle, apical vertebral translation, coronal balance, spinal length gain, etc. However, the SHILLA procedure experiences loss of correction or the reappearance of deformity through crankshafting or adding-on (e.g., distal migration). The current study identifies a solution with a modified approach to SHILLA (which could help in dynamically remodulating the apex of the deformity and mitigating loss of correction) and presents comparative correction data against the long-established traditional growth rod system.
The active apex correction (APC) group consisted of 20 patients and the growth rod group consisted of 26 patients, both with the same inclusion and exclusion criteria. The APC surgical procedure involved a modified SHILLA technique, that is, insertion of pedicle screws in the convex side of the vertebrae above and below the wedged one for compression and absence of apical fusion.
There were no statistical differences between the various spinal parameters (namely, Cobb angle, apical vertebral translation, sagittal balance, and spinal length gain) of the two groups. However, significant differences existed for coronal balance, which in part may have been due to differences in its pre-op value between the two groups.
APC and the traditional growth rod system showed similar deformity correction parameters at current follow-ups; however, the latter requires multiple surgeries to regularly distract the spine.
SHILLA手术和生长棒是早发性脊柱侧弯患者的两种主要手术矫正技术。这两种技术之间已经有一些比较研究,比较了诸如Cobb角、顶椎平移、冠状面平衡、脊柱长度增加等畸形识别特征。然而,SHILLA手术会因曲轴现象或附加现象(如远端移位)而出现矫正丢失或畸形复发。本研究确定了一种对SHILLA手术进行改良的方法(这有助于动态重塑畸形顶点并减轻矫正丢失),并给出了与长期使用的传统生长棒系统相比的矫正数据。
主动顶点矫正(APC)组有20例患者,生长棒组有26例患者,两组纳入和排除标准相同。APC手术采用改良的SHILLA技术,即在楔形椎体上下椎体的凸侧插入椎弓根螺钉进行加压,且不进行顶点融合。
两组的各种脊柱参数(即Cobb角、顶椎平移、矢状面平衡和脊柱长度增加)之间无统计学差异。然而,冠状面平衡存在显著差异,部分原因可能是两组术前值不同。
在目前的随访中,APC和传统生长棒系统显示出相似的畸形矫正参数;然而,后者需要多次手术来定期撑开脊柱。