Zheng Zheng, Guo Ying, Zou Chang-Peng
Department of Oncology, The First Hospital of Hebei Medical University, Shijiazhuang, China.
Medicine (Baltimore). 2020 Feb;99(7):e18332. doi: 10.1097/MD.0000000000018332.
Patients with advanced gastric or gastro-oesophageal junction cancer (GC/GEJC) that fail to respond to prior chemotherapy have poor clinical prognosis. Lately, many trials have paid much attention on the oncological outcomes of immune checkpoint inhibitors (ICI). A new therapy based on programmed death 1 (PD-1)/programmed death ligand 1 (PD-L1) inhibitors has recognized as promising prospects for advanced GC/GEJC. We assessed efficacy and safety of PD-L1 antibody versus chemotherapy alone in previously treated non-small cell lung cancer.
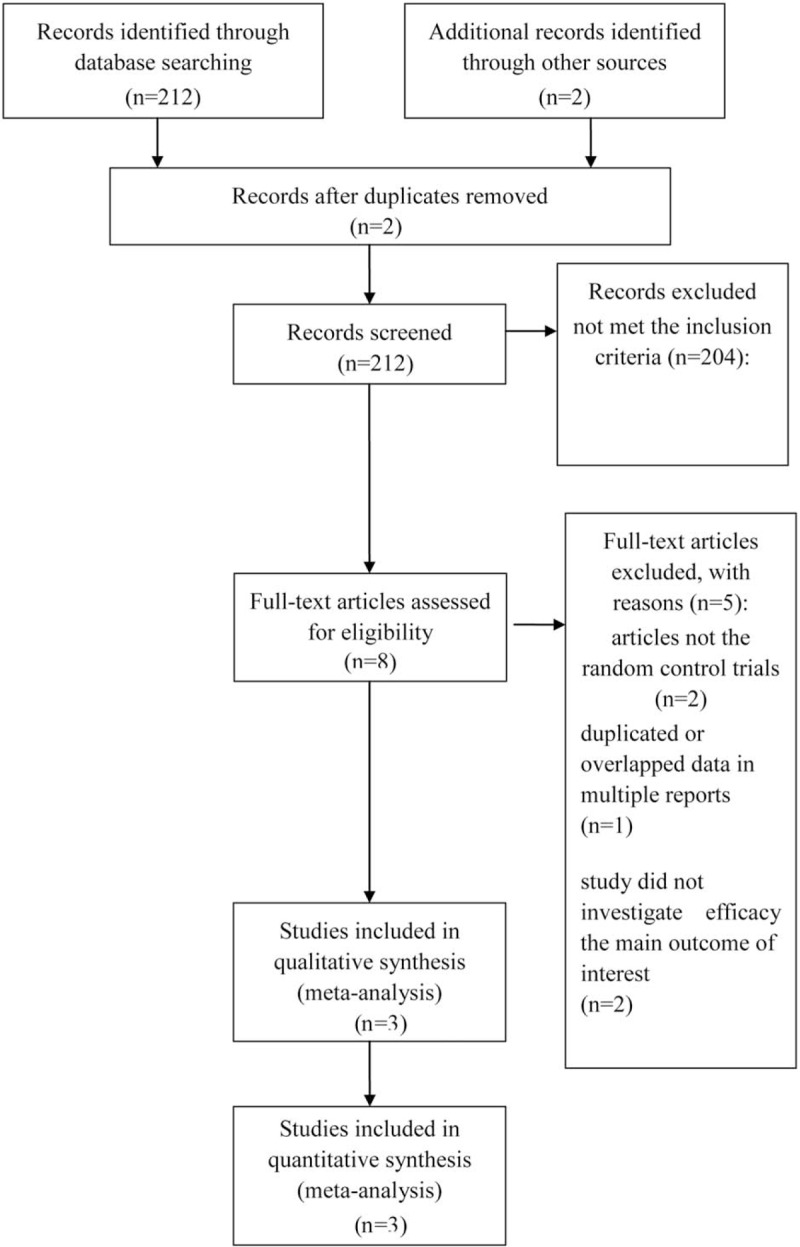
Computerized literature search was done on the published trials in: Pubmed, Embase, Cochrane library updated on June 2019. Randomized controlled trials were selected investigating chemotherapy plus PD-1/PD-L1 versus chemotherapy alone.
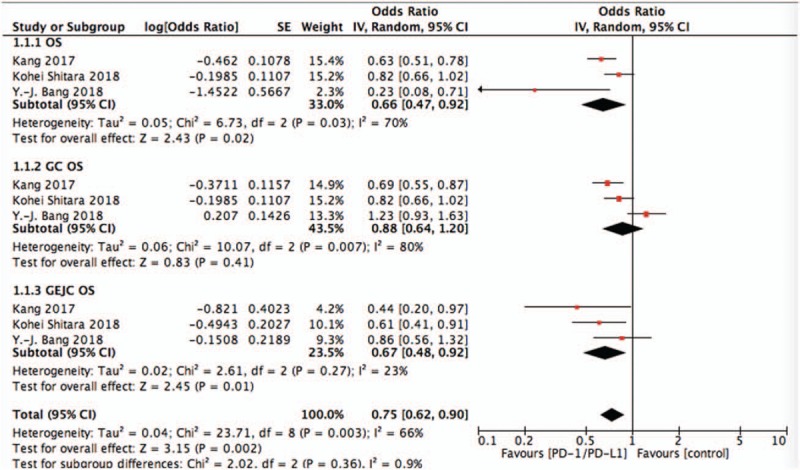
Three randomized controlled trails were included. The pooled analysis of overall survival (OS) was longer with anti-PD1/PD-L1 than with chemotherapy alone in the OS (OR = 0.66, 95%CI = 0.47-0.92, P = .02) and sub-group OS of GEJC (OR = 0.73, 95%CI = 0.58-0.93, P = .01). Whereas, there is no significant difference in progression-free survival (OR = 0.93, 95%CI = 0.62-1.39, P = .72). The pooling adverse events (AE) data did not achieve advantage in the PD-1/PD-L1 targeted agents (OR = 0.53, 95%CI = 0.13-2.10, P = .36), the same as the treatment-related AE of grade 3 to 5 (OR = 0.53, 95%CI = 0.16-1.74, P = .30).
Treatment of patients with advanced GC/GEJC with PD-1/PD-L1 targeted did result in an improvement in some but not all survival endpoints. Moreover, it had a comparable toxicity profile as compared with chemotherapy alone. More well designed studies are needed to develop a database of all anti-PD1/PD-L1 sub-groups and their individual impact on the differing anti-PD1/PD-L1 treatments.
对先前化疗无反应的晚期胃癌或胃食管交界癌(GC/GEJC)患者临床预后较差。近来,许多试验都非常关注免疫检查点抑制剂(ICI)的肿瘤学疗效。一种基于程序性死亡蛋白1(PD-1)/程序性死亡配体1(PD-L1)抑制剂的新疗法已被认为在晚期GC/GEJC治疗中具有广阔前景。我们评估了PD-L1抗体与单纯化疗相比在先前接受过治疗的非小细胞肺癌中的疗效和安全性。
对2019年6月更新的Pubmed、Embase、Cochrane图书馆中已发表的试验进行计算机文献检索。选择随机对照试验,比较化疗联合PD-1/PD-L1与单纯化疗的疗效。
纳入三项随机对照试验。在总生存期(OS)(OR = 0.66,95%CI = 0.47 - 0.92,P = 0.02)以及胃食管交界癌的亚组总生存期(OR = 0.73,95%CI = 0.58 - 0.93,P = 0.01)方面,抗PD1/PD-L1治疗组的总生存期长于单纯化疗组。然而,无进展生存期无显著差异(OR = 0.93,95%CI = 0.62 - 1.39,P = 0.72)。汇总的不良事件(AE)数据显示,PD-1/PD-L1靶向药物并无优势(OR = 0.53,95%CI = 0.13 - 2.10,P = 0.36),3至5级治疗相关不良事件情况也是如此(OR = 0.53,95%CI = 0.16 - 1.74,P = 0.30)。
使用PD-1/PD-L1靶向治疗晚期GC/GEJC患者确实在部分而非所有生存终点上有所改善。此外,与单纯化疗相比,其毒性特征相当。需要开展更多设计良好的研究,以建立所有抗PD1/PD-L1亚组及其对不同抗PD1/PD-L1治疗的个体影响的数据库。