Division of Oncology, Department of Medicine, University of Washington, Seattle, WA, USA.
Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA, USA.
Prostate Cancer Prostatic Dis. 2020 Sep;23(3):486-493. doi: 10.1038/s41391-020-0210-x. Epub 2020 Feb 13.
Cixutumumab, a monoclonal antibody targeting insulin-like growth factor I receptor, did not improve undetectable prostate-specific antigen (PSA) rate at 28 weeks when combined with androgen deprivation in the randomized phase II SWOG S0925 trial for patients with new metastatic hormone-sensitive prostate cancer. We now present mature survival analyses, along with pre-specified secondary and exploratory endpoints.
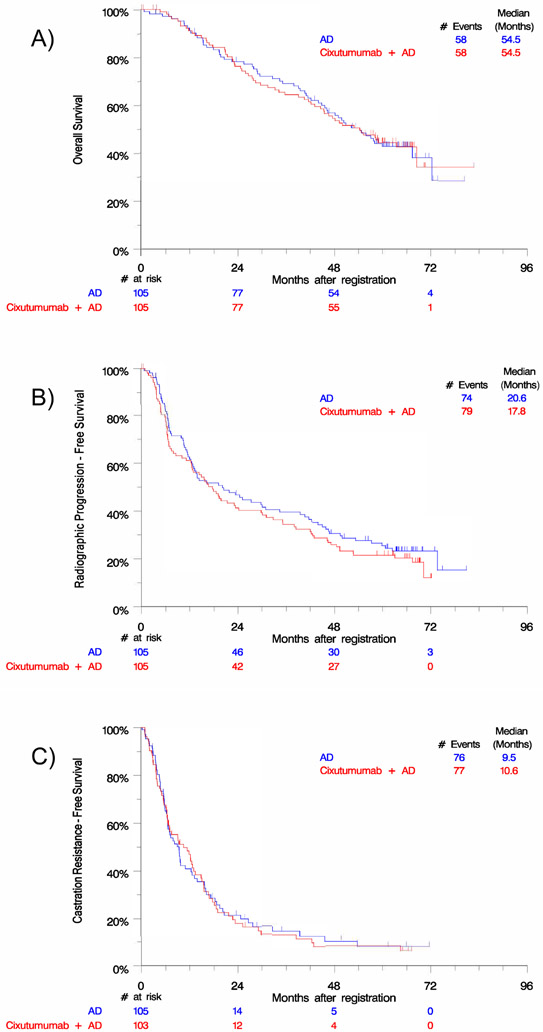
We randomized 210 patients to androgen deprivation with or without cixutumumab, 105 per treatment arm. We used Kaplan-Meier curves to analyze overall survival, radiographic progression-free survival, and castration resistance-free survival by treatment arm, disease volume, and risk group. We explored differences in survival by treatment arm via covariate-adjusted Cox proportional hazards models adjusted for disease volume and risk.
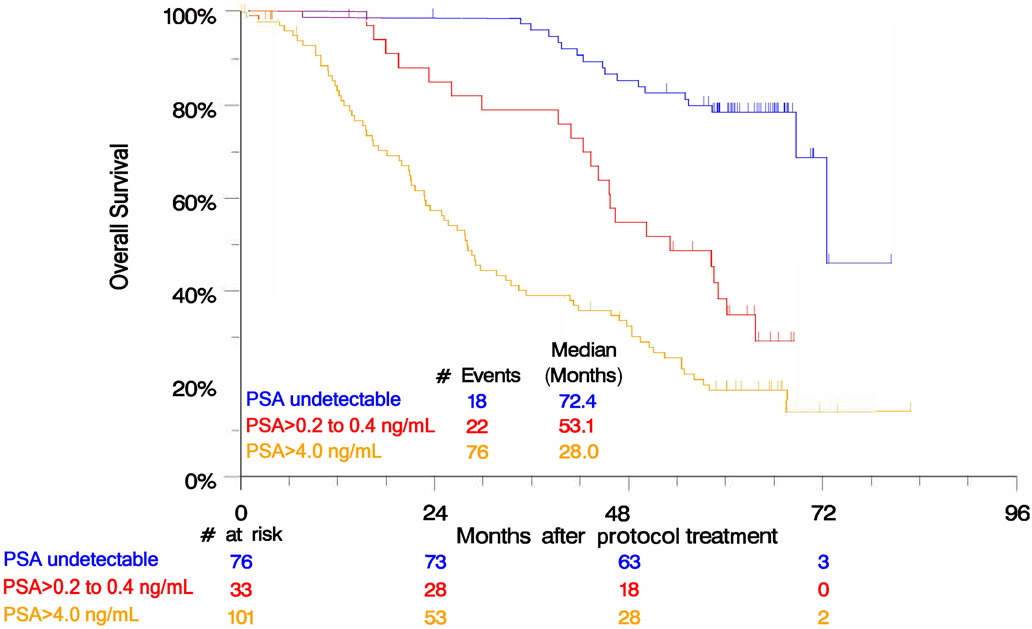
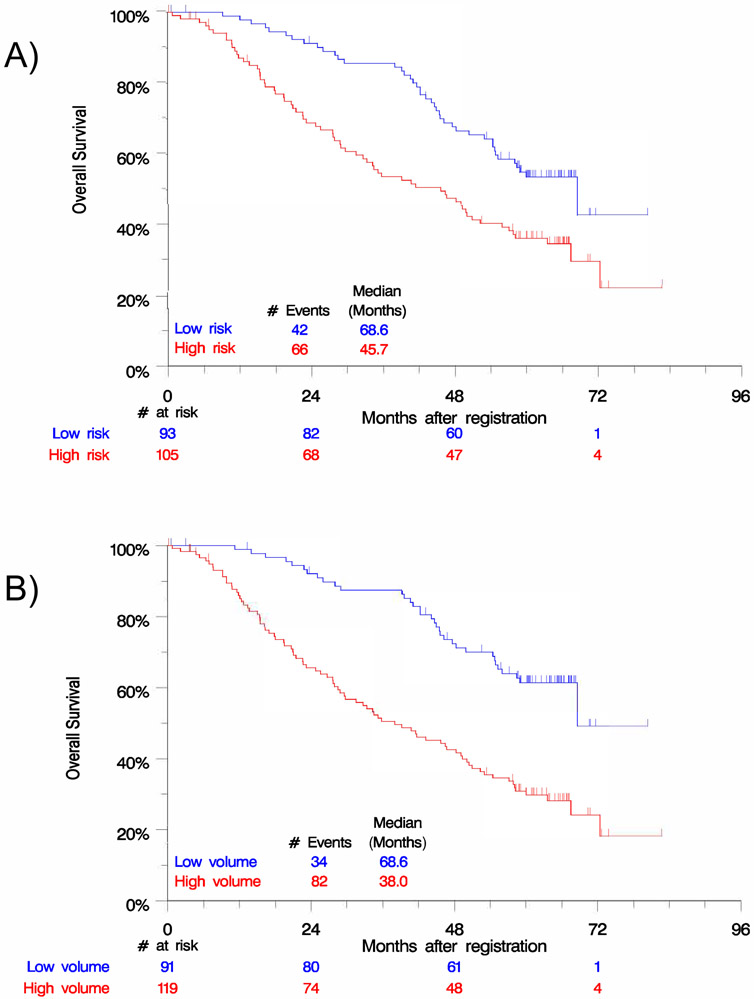
No difference was seen between treatment arms in overall survival (HR 1.01 [0.70-1.45]; p = 0.97), radiographic progression-free survival (HR 1.17 [0.85-1.60]; p = 0.35), or castration resistance-free survival (HR 1.02 [0.75-1.41]; p = 0.88). At baseline, 105/198 (53.0%) patients had high-risk features and 119/210 (56.7%) had high-volume disease; 16.7% of patients had discordant classifications of high or low category for risk and volume. Adjusting for risk or volume yielded no differences in overall survival between arms. Inferior survival was observed in high-risk (HR 1.89 [1.29-2.80]; p = 0.001) and high-volume (HR 2.75 [1.84-4.10]; p < 0.0001) disease. Disease volume was a better fit to survival data than risk group (AIC 878.3 vs. 889.2). Compared to patients achieving undetectable PSA at 28 weeks, inferior survival was observed in patients whose PSA was >0.2 to ≤4.0 ng/mL (HR 3.72 [1.99-6.95]; p < 0.0001) or >4.0 ng/mL (HR 7.13 [4.24-11.9]; p < 0.0001).
In new metastatic hormone-sensitive prostate cancer, addition of cixutumumab to androgen deprivation did not improve survival. Baseline risk and disease volume carried prognostic value for this distinct trial population, although disease volume added more prognostic information. PSA treatment response was a strong intermediate endpoint for survival.
在新诊断转移性去势敏感性前列腺癌患者中,西妥昔单抗联合雄激素剥夺治疗未能提高 28 周时不可检测的前列腺特异性抗原(PSA)率,SWOG S0925 试验是一项随机的 II 期试验。目前我们提供成熟的生存分析结果,以及预先设定的次要终点和探索性终点。
我们将 210 例患者随机分为雄激素剥夺治疗加或不加西妥昔单抗组,每组 105 例。我们使用 Kaplan-Meier 曲线分析按治疗组、疾病体积和风险组的总生存、影像学无进展生存和去势抵抗无进展生存。我们通过协变量调整 Cox 比例风险模型,按治疗组、疾病体积和风险组调整生存差异。
两组总生存(HR 1.01[0.70-1.45];p=0.97)、影像学无进展生存(HR 1.17[0.85-1.60];p=0.35)或去势抵抗无进展生存(HR 1.02[0.75-1.41];p=0.88)无差异。基线时,198 例患者中有 105 例(53.0%)具有高危特征,210 例中有 119 例(56.7%)具有高肿瘤体积;16.7%的患者具有风险和体积高低分类的不一致性。按风险或体积调整后,两组总生存无差异。高危(HR 1.89[1.29-2.80];p=0.001)和高肿瘤体积(HR 2.75[1.84-4.10];p<0.0001)疾病患者的生存情况更差。与 28 周时 PSA 不可检测的患者相比,PSA 为 0.2~4.0ng/ml(HR 3.72[1.99-6.95];p<0.0001)或>4.0ng/ml(HR 7.13[4.24-11.9];p<0.0001)的患者生存情况更差。
在新诊断的转移性去势敏感性前列腺癌中,西妥昔单抗联合雄激素剥夺治疗并未改善生存。在这个特定的试验人群中,基线风险和疾病体积具有预后价值,尽管疾病体积提供了更多的预后信息。PSA 治疗反应是生存的一个强有力的中间终点。