Parthasarathy Rajsrinivas, Gupta Vipul
Department of Stroke and Neurointerventional Surgery, Artemis Agrim Institute of Neuroscience, Gurgaon, India.
Ann Indian Acad Neurol. 2020 Jan-Feb;23(1):13-19. doi: 10.4103/aian.AIAN_359_19.
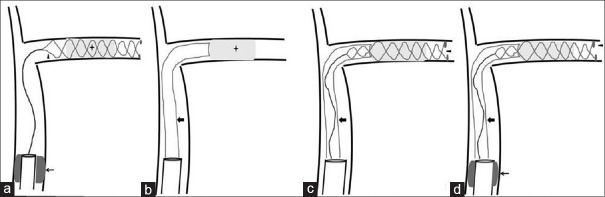
The stroke physician community witnessed a major "breakthrough" in acute stroke therapeutics when the results of the first of the many positive trials, "MR CLEAN," were published showing a significant absolute benefit in favor of mechanical thrombectomy in patients with large vessel occlusion (LVO). Thereafter, the investigators of ESCAPE, SWIFT PRIME, REVASCAT, THRACE, and PISTE concluded the same. Based on the initial studies, the American Stroke Association amended the 2013 guidelines in 2015 to include mechanical thrombectomy as the standard of care in patients with LVO presenting within six hours. In the past year, the horizon was further expanded when two major landmark trials, DAWN and DEFUSE 3, established the benefit of mechanical thrombectomy in the delayed window period in a select group of patients. It further led to the inclusion of the delayed window period treatment strategies in the 2018 guidelines. However, there are many unanswered questions in scenarios like small deficit with LVO, borderline large core, wake-up stroke (WUS), tandem occlusion, imaging of choice, conscious sedation (CS) versus general anesthesia (GA), and choice of technique. In our review, we aim to answer these questions along with a schematic representation of current techniques used in stroke thrombectomy.
当众多阳性试验中的首个试验“MR CLEAN”的结果公布,显示对大血管闭塞(LVO)患者进行机械取栓有显著的绝对获益时,卒中内科医生群体见证了急性卒中治疗领域的一项重大“突破”。此后,“ESCAPE”“SWIFT PRIME”“REVASCAT”“THRACE”和“PISTE”的研究人员也得出了相同结论。基于这些初步研究,美国卒中协会在2015年修订了2013年的指南,将机械取栓纳入6小时内就诊的LVO患者的标准治疗方法。在过去一年里,两项具有里程碑意义的大型试验“DAWN”和“DEFUSE 3”证实了在特定患者群体的延迟窗口期进行机械取栓的获益,这进一步拓展了视野。这也使得延迟窗口期治疗策略被纳入2018年的指南。然而,在诸如LVO伴小缺损、临界大梗死核心、醒后卒中(WUS)、串联闭塞、成像选择、清醒镇静(CS)与全身麻醉(GA)以及技术选择等情况下,仍有许多问题未得到解答。在我们的综述中,我们旨在回答这些问题,并以示意图展示目前用于卒中取栓的技术。