Chaudhuri Dipayan, Bishay Kirles, Tandon Parul, Trivedi Vatsal, James Paul D, Kelly Erin M, Thavorn Kednapa, Kyeremanteng Kwadwo
Department of Critical Care McMaster University Hamilton Ontario Canada.
Department of Gastroenterology University of Toronto Toronto Ontario Canada.
JGH Open. 2019 May 24;4(1):22-28. doi: 10.1002/jgh3.12195. eCollection 2020 Feb.
Prophylactic endotracheal intubation for airway protection prior to endoscopy for the management of severe upper gastrointestinal bleeding (UGIB) is controversial. The aim of this meta-analysis is to examine the clinical outcomes and costs related to prophylactic endotracheal intubation compared to no intubation in UGIB.
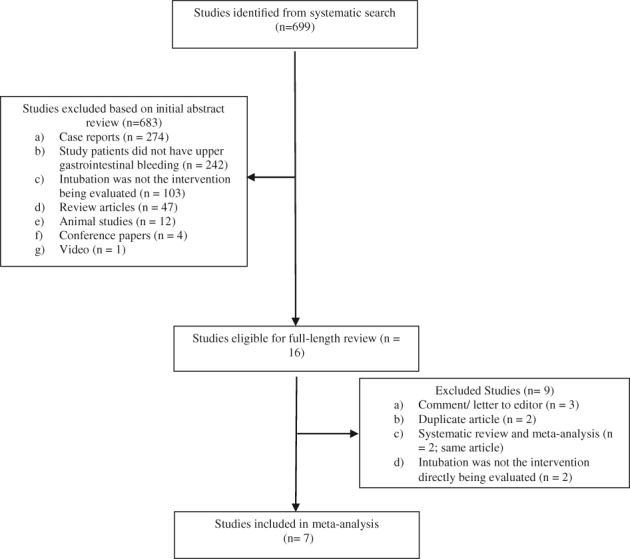
EMBASE, MEDLINE, and the Cochrane Central Register of Controlled Trials were used to identify studies through June 2017. Data regarding mortality, total hospital and intensive care unit length of stay (LOS), pneumonia, and cardiovascular events were collected. The DerSimonian-Laird random effects models were used to calculate the inverse variance-based weighted, pooled treatment effect across studies.
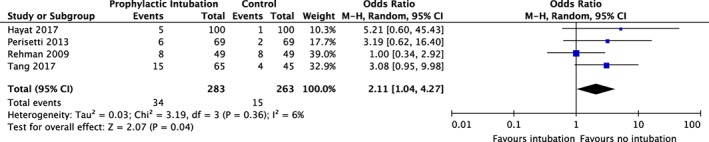
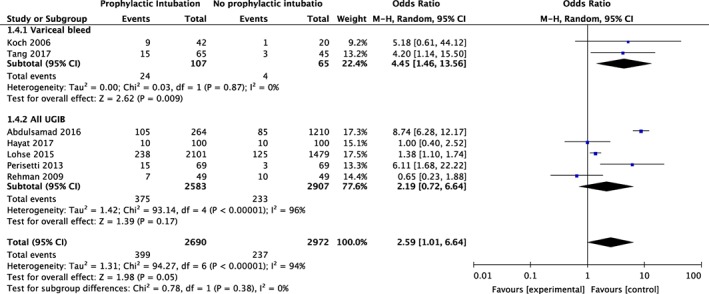
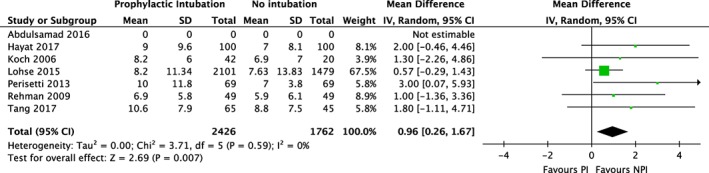
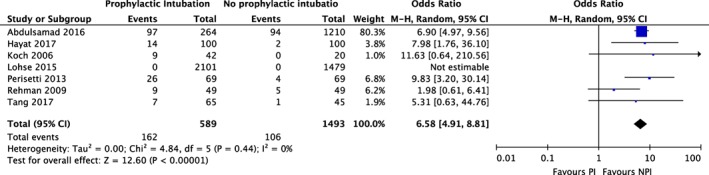
Seven studies (five manuscripts and two abstracts) were identified (5662 total patients). Prophylactic intubation conferred an increased risk of death (odds ratio [OR], 2.59, 95% confidence interval [CI]: 1.01-6.64), hospital LOS (mean difference, 0.96 days, 95% CI: 0.26-1.67), and pneumonia (OR 6.58, 95% CI: 4.91-8.81]) compared to endoscopy without intubation. The LOS-related cost was greater when prophylactic intubation was performed ($9020 per patient, 95% CI: $6962-10 609) compared to when it was not performed ($7510 per patient, 95% CI: $6486-8432). There was no difference in risk of cardiovascular events after sensitivity analysis.
Prophylactic intubation in severe UGIB is associated with a greater risk of pneumonia, LOS, death, and cost compared to endoscopy without intubation. Randomized trials examining this issue are warranted.
在内镜检查前进行预防性气管插管以保护气道用于严重上消化道出血(UGIB)的处理存在争议。本荟萃分析的目的是探讨与不插管相比,预防性气管插管在UGIB中的临床结局和成本。
使用EMBASE、MEDLINE和Cochrane对照试验中央注册库检索截至2017年6月的研究。收集有关死亡率、总住院时间和重症监护病房住院时间(LOS)、肺炎和心血管事件的数据。采用DerSimonian-Laird随机效应模型计算各研究基于逆方差的加权合并治疗效应。
共纳入7项研究(5篇手稿和2篇摘要)(共5662例患者)。与未插管的内镜检查相比,预防性插管增加了死亡风险(比值比[OR]为2.59,95%置信区间[CI]:1.01 - 6.64)、住院LOS(平均差为0.96天,95%CI:0.26 - 1.67)和肺炎风险(OR为6.58,95%CI:4.91 - 8.81)。与未进行预防性插管时(每位患者7510美元,95%CI:6486 - 8432美元)相比,进行预防性插管时与LOS相关的成本更高(每位患者9020美元,95%CI:6962 - 10609美元)。敏感性分析后心血管事件风险无差异。
与未插管的内镜检查相比,严重UGIB中的预防性插管与更高风险的肺炎、LOS、死亡和成本相关。有必要进行随机试验来研究这个问题。