Pasha Syed Bilal, Tarar Zahid Ijaz, Chela Harleen, McDermott Aidan, Ihnat Jocelyn, Matteson-Kome Michelle L, Ghouri Yezaz A, Bechtold Matthew L
Gastroenterology and Hepatology, University of Missouri, Columbia, USA.
Internal Medicine, University of Missouri, Columbia, USA.
Cureus. 2024 Jul 15;16(7):e64567. doi: 10.7759/cureus.64567. eCollection 2024 Jul.
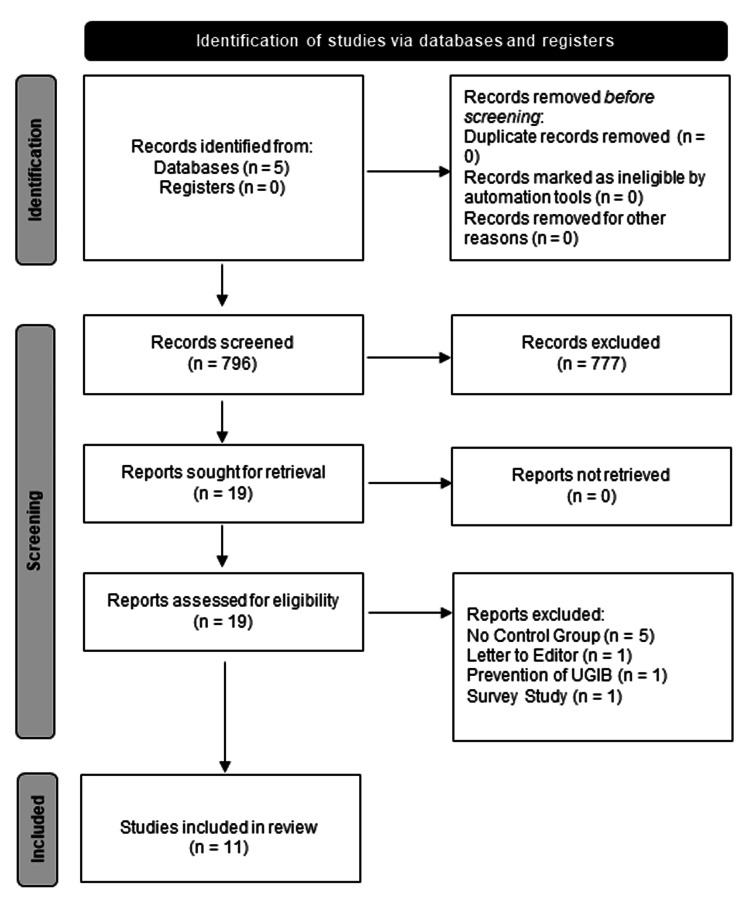
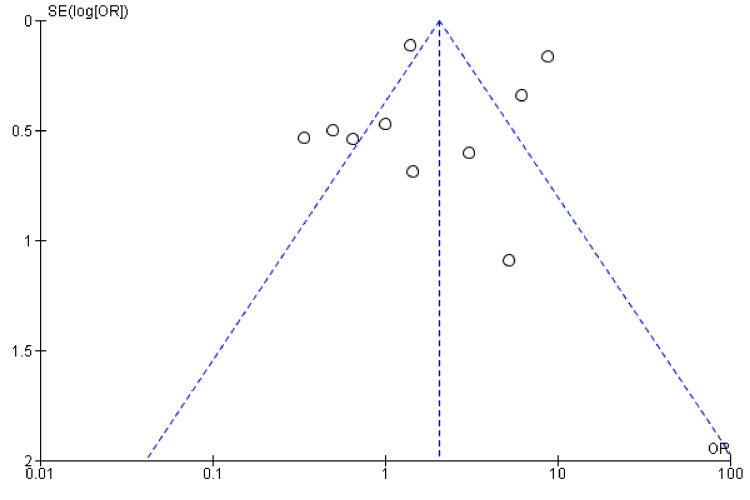
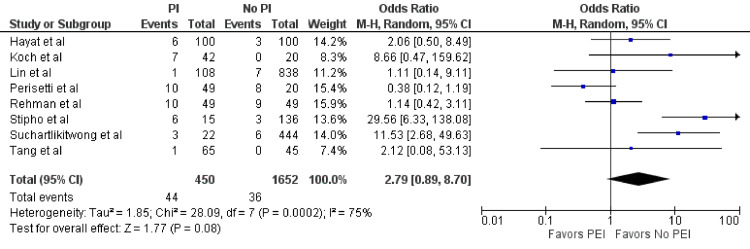
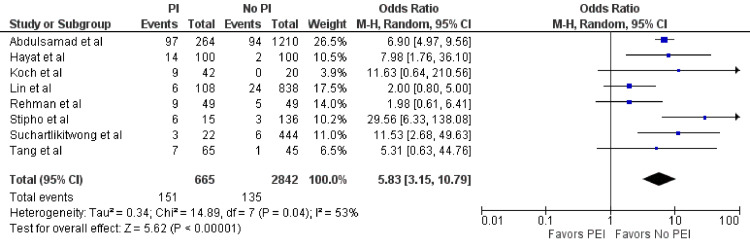
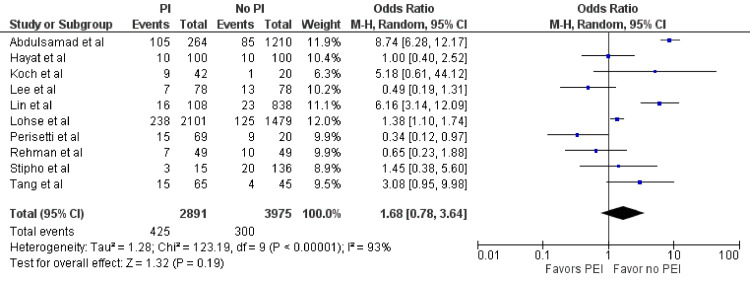
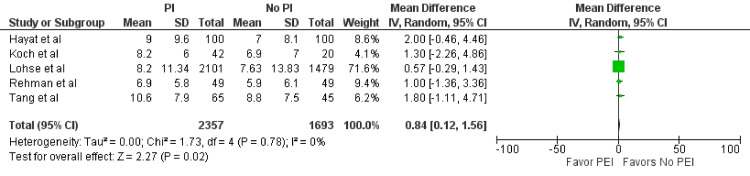
No consensus exists on the standard of intraoperative airway management approach to prevent endoscopy complications in acute gastrointestinal (GI) bleeding. Eight years after our initial meta-analysis, we reassessed the effect of prophylactic endotracheal intubation in acute GI bleeding in hospitalized patients. Multiple databases were reviewed in 2024, identifying 10 studies that compared prophylactic endotracheal intubation (PEI) versus no intubation in acute upper GI bleeding in hospitalized patients. Outcomes of interest included pneumonia, length of hospital stay, aspiration, and mortality. The odds ratio (OR) or mean difference (MD) using the random effects model was calculated for each outcome. In total, 11 studies (10 retrospective, one prospective) were included in the meta-analysis (n = 7,332). PEI demonstrated statistically significant higher odds of pneumonia (OR = 5.83; 95% confidence interval (CI) = 3.15-10.79; p < 0.01) and longer length of stays (MD = 0.84; 95% CI = 0.12-1.56; p = 0.02). However, mortality (OR = 1.68; 95% CI = 0.78-3.64; p = 0.19) and aspiration (OR = 2.79; 95% CI = 0.89-8.7; p = 0.08) were not statistically significant. PEI before esophagogastroduodenoscopy for hospitalized upper GI bleeding patients is associated with an increased incidence of pneumonia within 48 hours and prolonged hospitalization but no statistically significant increased risk of mortality or aspiration.
关于预防急性胃肠道(GI)出血内镜检查并发症的术中气道管理方法标准,目前尚无共识。在我们最初的荟萃分析八年后,我们重新评估了预防性气管插管对住院患者急性胃肠道出血的影响。2024年对多个数据库进行了回顾,确定了10项比较预防性气管插管(PEI)与未插管对住院患者急性上消化道出血影响的研究。感兴趣的结局包括肺炎、住院时间、误吸和死亡率。对每个结局使用随机效应模型计算比值比(OR)或平均差(MD)。总共11项研究(10项回顾性研究,1项前瞻性研究)纳入了荟萃分析(n = 7,332)。PEI显示肺炎发生率具有统计学显著更高的OR值(OR = 5.83;95%置信区间(CI)= 3.15 - 10.79;p < 0.01),住院时间更长(MD = 0.84;95% CI = 0.12 - 1.56;p = 0.02)。然而,死亡率(OR = 1.68;95% CI = 0.78 - 3.64;p = 0.19)和误吸(OR = 2.79;95% CI = 0.89 - 8.7;p = 0.08)无统计学显著差异。对于住院的上消化道出血患者,在食管胃十二指肠镜检查前进行PEI与48小时内肺炎发生率增加和住院时间延长相关,但死亡率或误吸风险无统计学显著增加。