O'Sullivan Brian, Hui Huang Shao, Keane Thomas, Xu Wei, Su Jie, Waldron John, Gullane Patrick, Liu Fei-Fei, Warde Padraig, Payne David, Tong Li, Cummings Bernard
Department of Radiation Oncology, Princess Margaret Cancer Centre, University of Toronto, Canada.
Department of Otolaryngology-Head and Neck Surgery, Princess Margaret Cancer Centre, University of Toronto, Canada.
Clin Transl Radiat Oncol. 2020 Jan 28;21:69-76. doi: 10.1016/j.ctro.2020.01.003. eCollection 2020 Mar.
PURPOSE/OBJECTIVES: To examine the therapeutic ratio and mortality profile over time in a radiotherapy randomized trial in stage III-IV larynx/pharynx cancer with long-term follow-up.
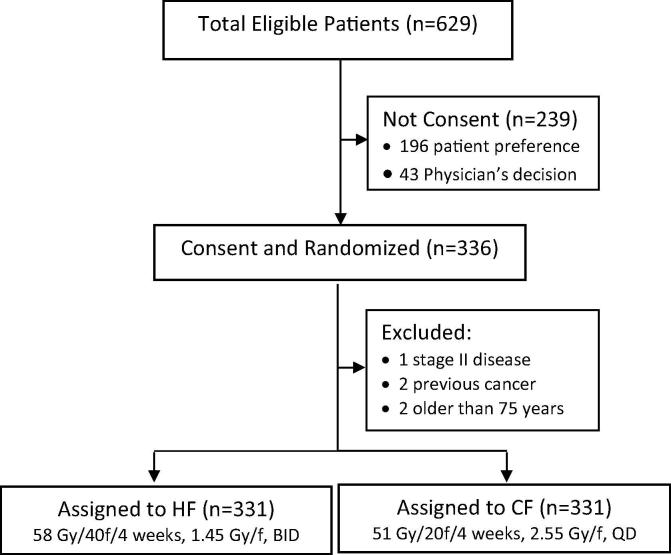
MATERIALS/METHODS: From 1988 to 1995, 331 cases were randomized to either hyperfractionated (HF) (58 Gy/40 fractions, twice daily) or conventional (CF) (51 Gy/20 fractions, once daily) radiotherapy. Overall survival (OS), locoregional (LRC), distant control (DC), ≥Grade 3 late toxicity (LT), and relative mortality risk profile over time were compared between both arms.
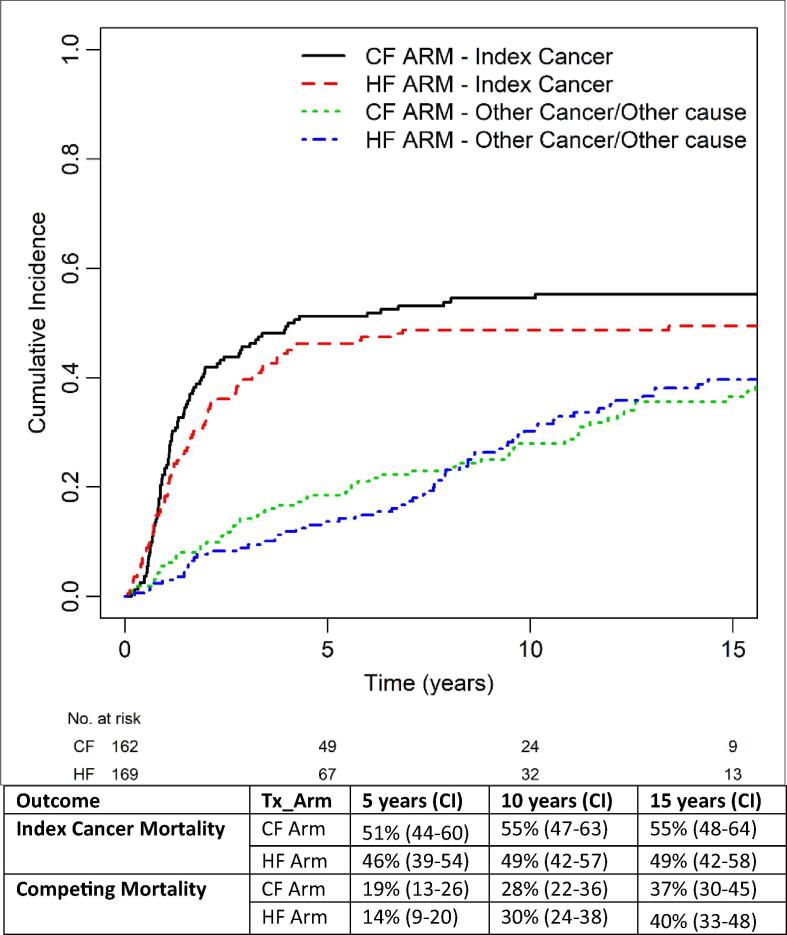
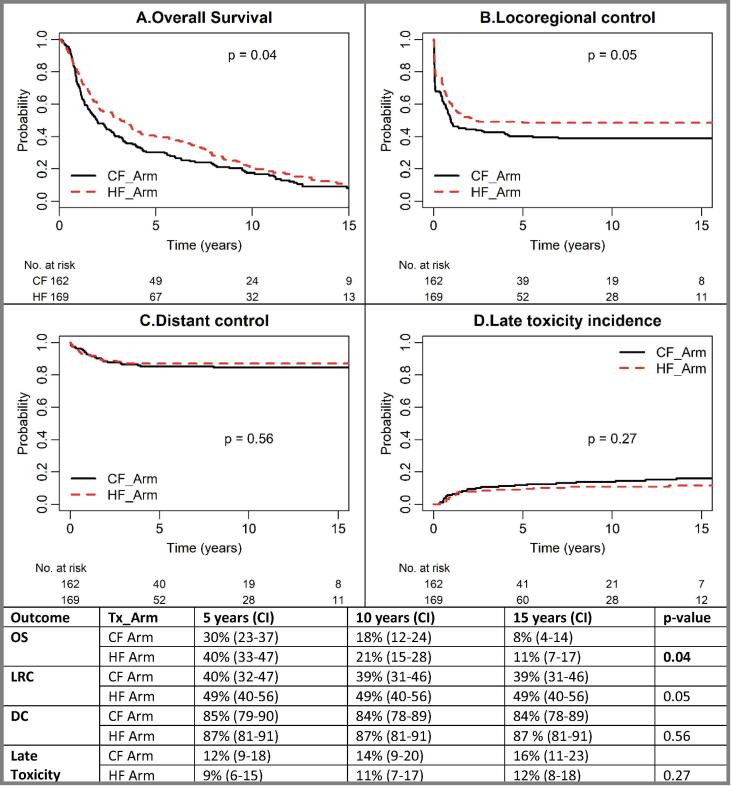
Median follow-up was 13.6 years. HF had a 10% improved OS at 5-years (40% vs 30%, p = 0.04), but the benefit diminished to 3% at 10-years (21% vs 18%). A trend towards higher LRC with HF remained (5-year: 49% vs 40%; 10-year: 49% vs 39%, p = 0.05). DC rates were unchanged (5-year: 87% vs 85%; 10-year: 87 vs 84%, p = 0.56). LT rates were similar (HF vs CF: 5-year: 9% vs 12%; 10-year: 11% vs 14%, p = 0.27). Multivariable analysis confirmed that HF reduced mortality risk by 31% [HR 0.69 (0.55-0.88), p < 0.01] and locoregional failure risk by 35% [HR 0.65 (0.48-0.89), p < 0.01]. Index cancer mortality (5-year: 46% vs 51%; 10-year: 49% vs 55%) was lower in the HF arm. Competing mortality (mostly smoking-related) was also numerically lower with HF at 5-years (14% vs 19%) but became similar at 10-years (30% vs 28%).
This trial confirms that HF with augmented total dose has a durable 10% effect size on LRC with comparable LT. OS benefit is evident at 5-years (10%) but relative mortality risk profile changes in longer follow-up.
目的/目标:在一项针对III-IV期喉/咽癌的放疗随机试验中,进行长期随访,以研究治疗比和随时间变化的死亡率情况。
材料/方法:1988年至1995年,331例患者被随机分为超分割放疗组(HF)(58 Gy/40次,每日两次)或常规放疗组(CF)(51 Gy/20次,每日一次)。比较两组的总生存率(OS)、局部区域控制率(LRC)、远处控制率(DC)、≥3级晚期毒性反应(LT)以及随时间变化的相对死亡风险情况。
中位随访时间为13.6年。超分割放疗组在5年时总生存率提高了10%(40%对30%,p = 0.04),但在10年时获益降至3%(21%对18%)。超分割放疗组局部区域控制率仍有升高趋势(5年:49%对40%;10年:49%对39%,p = 0.05)。远处控制率无变化(5年:87%对85%;10年:87对84%,p = 0.56)。晚期毒性反应率相似(超分割放疗组对常规放疗组:5年:9%对12%;10年:11%对14%,p = 0.27)。多变量分析证实,超分割放疗使死亡风险降低31%[风险比(HR)0.69(0.55 - 0.88),p < 0.01],局部区域失败风险降低35%[HR 0.65(0.48 - 0.89),p < 0.01]。超分割放疗组的指数癌症死亡率较低(5年:46%对51%;10年:49%对55%)。5年时超分割放疗组的竞争性死亡率(大多与吸烟相关)在数值上也较低(14%对19%),但在10年时变得相似(30%对28%)。
该试验证实,增加总剂量的超分割放疗对局部区域控制有持久的10%的效应大小,且晚期毒性反应相当。5年时总生存率获益明显(10%),但在更长随访期内相对死亡风险情况发生变化。