Department of Cardiovascular Medicine, Kyoto University Graduate School of Medicine and Faculty of Medicine, Kyoto, Japan.
Department of Cardiology, Mitsubishi Kyoto Hospital, Kyoto, Japan.
BMJ Open. 2020 Feb 16;10(2):e032674. doi: 10.1136/bmjopen-2019-032674.
To investigate the prevalence and risk factors of functional decline during hospitalisation and its relationship with postdischarge outcomes in very old patients with acute decompensated heart failure (ADHF) hospitalisation.
Prospective cohort study between 1 October 2014 and 31 March 2016.
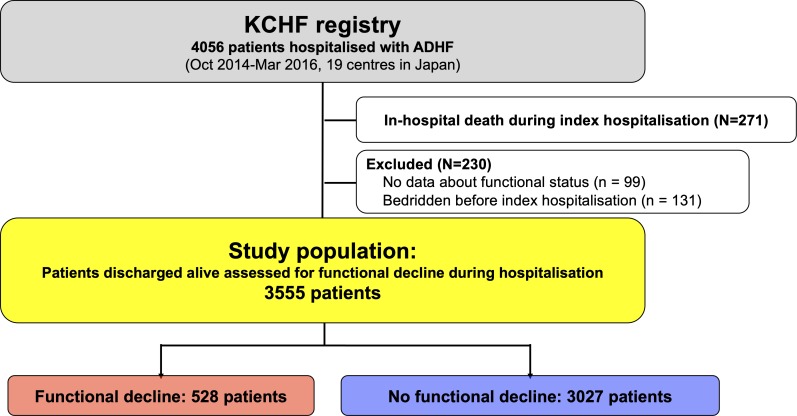
A physician-initiated, multicentre study of consecutive patients admitted for ADHF in 19 hospitals throughout Japan.
Among 3555 patients hospitalised for ADHF (median age (IQR), 80 (71-86) years; 1572 (44%) women), functional decline during the index hospitalisation occurred in 528 patients (15%).
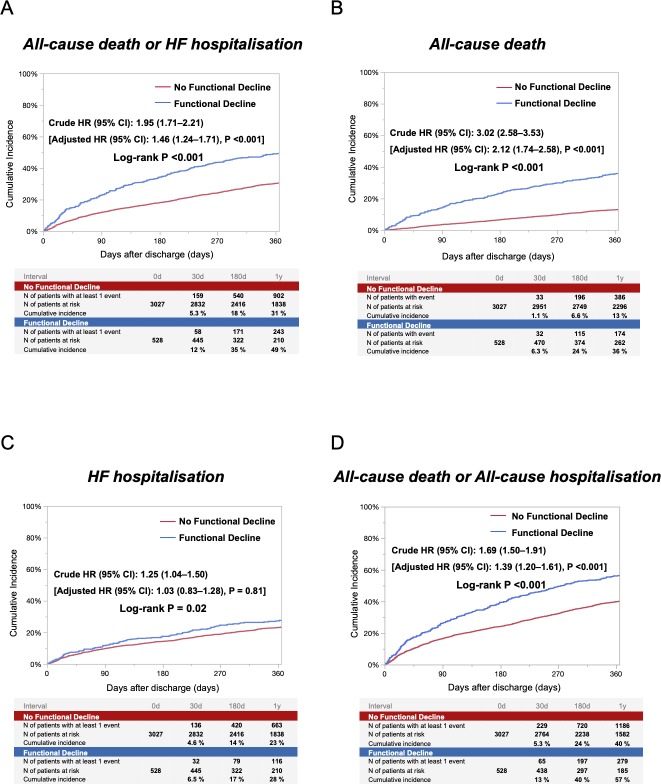
The primary outcome measure was a composite of all-cause death or heart failure (HF) hospitalisation after discharge. The secondary outcome measures were all-cause death, HF hospitalisation, and a composite of all-cause death or all-cause hospitalisation.
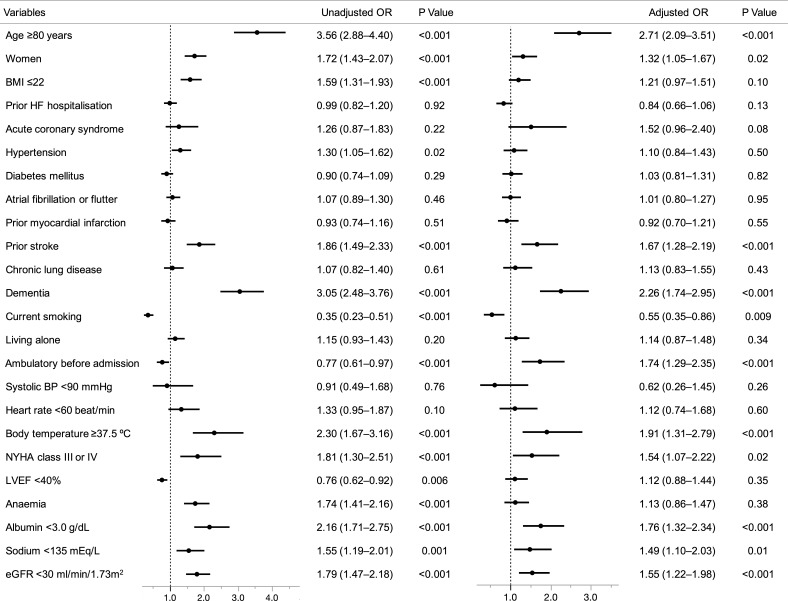
The independent risk factors for functional decline included age ≥80 years (OR 2.71; 95% CI 2.09 to 3.51), female (OR 1.32; 95% CI 1.05 to 1.67), prior stroke (OR 1.67; 95% CI 1.28 to 2.19), dementia (OR 2.26; 95% CI 1.74 to 2.95), ambulatory before admission (OR 1.74; 95% CI 1.29 to 2.35), elevated body temperature (OR 1.91; 95% CI 1.31 to 2.79), New York Heart Association class III or IV on admission (OR 1.54; 95% CI 1.07 to 2.22), decreased albumin levels (OR 1.76; 95% CI 1.32 to 2.34), hyponatraemia (OR 1.49; 95% CI 1.10 to 2.03) and renal dysfunction (OR 1.55; 95% CI 1.22 to 1.98), after multivariable adjustment. The cumulative 1-year incidence of the primary outcome in the functional decline group was significantly higher than that in the no functional decline group (50% vs 31%, log-rank p<0.001). After adjusting for baseline characteristics, the higher risk of the functional decline group relative to the no functional decline group remained significant (adjusted HR 1.46; 95% CI 1.24 to 1.71; p<0.001).
Independent risk factors of functional decline in very old patients with ADHF were related to both frailty and severity of HF. Functional decline during ADHF hospitalisation was associated with unfavourable postdischarge outcomes.
NCT02334891, UMIN000015238.
调查急性失代偿性心力衰竭(ADHF)住院期间功能下降的患病率和危险因素及其与出院后结局的关系。
2014 年 10 月 1 日至 2016 年 3 月 31 日期间进行的前瞻性队列研究。
日本 19 家医院的医生发起的多中心 ADHF 连续患者研究。
在因 ADHF 住院的 3555 名患者中(中位数(IQR)年龄 80(71-86)岁;1572 名[44%]女性),528 名(15%)患者在指数住院期间出现功能下降。
主要结局指标为出院后全因死亡或心力衰竭(HF)住院的复合结局。次要结局指标为全因死亡、HF 住院和全因死亡或全因住院的复合结局。
功能下降的独立危险因素包括年龄≥80 岁(OR 2.71;95%CI 2.09 至 3.51)、女性(OR 1.32;95%CI 1.05 至 1.67)、既往卒中(OR 1.67;95%CI 1.28 至 2.19)、痴呆(OR 2.26;95%CI 1.74 至 2.95)、入院前活动能力(OR 1.74;95%CI 1.29 至 2.35)、体温升高(OR 1.91;95%CI 1.31 至 2.79)、入院时纽约心脏协会心功能 III 或 IV 级(OR 1.54;95%CI 1.07 至 2.22)、白蛋白水平降低(OR 1.76;95%CI 1.32 至 2.34)、低钠血症(OR 1.49;95%CI 1.10 至 2.03)和肾功能不全(OR 1.55;95%CI 1.22 至 1.98),在多变量调整后。功能下降组的 1 年累积主要结局发生率明显高于无功能下降组(50% vs 31%,log-rank p<0.001)。在调整基线特征后,功能下降组相对于无功能下降组的高风险仍然显著(调整后的 HR 1.46;95%CI 1.24 至 1.71;p<0.001)。
ADHF 高龄患者功能下降的独立危险因素与衰弱和 HF 严重程度均有关。ADHF 住院期间的功能下降与出院后不良结局相关。
NCT02334891,UMIN000015238。