Vaegter Henrik Bjarke, Ussing Kaper, Johansen Jannick Vaaben, Stegemejer Irene, Palsson Thorvaldur Skuli, O'Sullivan Peter, Kent Peter
Pain Research Group, Pain Center, Department of Anesthesiology and Intensive Care Medicine, Odense University Hospital, Denmark.
Department of Clinical Research, Faculty of Health Sciences, University of Southern Denmark, Odense, Denmark.
Pain Rep. 2019 Dec 17;5(1):e802. doi: 10.1097/PR9.0000000000000802. eCollection 2020 Jan-Feb.
Multidisciplinary care is recommended for disabling persistent low back pain (pLBP) nonresponsive to primary care. Cognitive functional therapy (CFT) is a physiotherapy-led individualised intervention targeting psychological, physical, and lifestyle barriers to recovery, to self-manage pLBP.
This pilot study investigated clinical outcomes and pain thresholds after a 12-week CFT pathway in patients with severe pLBP referred to a University Pain Center. Exploratory analyses compared changes in clinical outcomes, opioid consumption, and costs after CFT with changes after a multidisciplinary pain management (MPM) pathway.
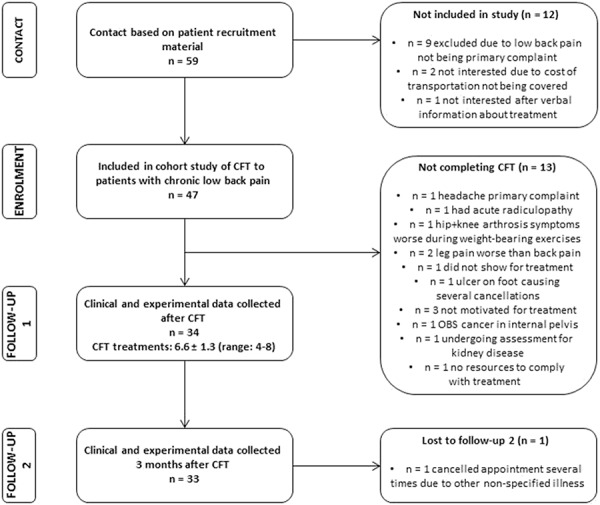
In total, 47 consecutively referred pLBP patients consented to the CFT pathway. At baseline, 3 and 6 months, clinical outcomes and PPTs were assessed. Control patients (n = 99) who had completed an MPM pathway in the last 3 years were matched from the clinical pain registry used in the Pain Center in a 3:1 ratio based on propensity scores derived from relevant baseline variables of the CFT cases.
Most clinical outcomes and low back pressure pain threshold were improved at 3 and 6 months after the CFT pathway. Compared with MPM, CFT patients had significantly larger reductions in disability and improved quality of life after the interventions at a lower cost (-3688€ [confidence interval: -3063 to -4314€]). Reduction in pain intensity and proportion of patients withdrawing from opioids (18.2% vs 27.8%) were similar between CFT and MPM groups.
Improvements in clinical and experimental pain were found after the CFT pathway. Fully powered randomized controlled trials comparing CFT with an MPM program in patients with disabling pLBP are warranted to control for the current limitations.
对于初级保健无反应的致残性持续性下腰痛(pLBP),推荐采用多学科护理。认知功能疗法(CFT)是一种以物理治疗为主导的个体化干预措施,针对心理、身体和生活方式等影响康复的障碍,以自我管理pLBP。
本试点研究调查了转诊至大学疼痛中心的重度pLBP患者在接受为期12周的CFT治疗后的临床结局和疼痛阈值。探索性分析比较了CFT治疗后与多学科疼痛管理(MPM)治疗后临床结局、阿片类药物消耗和成本的变化。
共有47例连续转诊的pLBP患者同意接受CFT治疗。在基线、3个月和6个月时,评估临床结局和疼痛阈值。根据CFT病例的相关基线变量得出的倾向评分,从疼痛中心使用的临床疼痛登记册中按3:1的比例匹配在过去3年中完成MPM治疗的对照患者(n = 99)。
在CFT治疗后的3个月和6个月,大多数临床结局和下背压痛阈值得到改善。与MPM相比,CFT患者在干预后残疾程度显著降低,生活质量改善,成本更低(-3688欧元[置信区间:-3063至-4314欧元])。CFT组和MPM组在疼痛强度降低和停用阿片类药物的患者比例(18.2%对27.8%)方面相似。
CFT治疗后临床和实验性疼痛均有改善。有必要进行充分有力的随机对照试验,比较CFT与MPM方案在致残性pLBP患者中的效果,以控制当前的局限性。