Pathology, Institut Jules Bordet, Université Libre de Bruxelles, Bruxelles, Belgium.
Pathology, Hôpital Erasme, Université Libre de Bruxelles, Bruxelles, Belgium.
BMC Cancer. 2020 Feb 19;20(1):135. doi: 10.1186/s12885-020-6613-1.
Immunotherapy represents a promising option for treatment of hepatocellular carcinoma (HCC) in cirrhotic patients but its efficacy is currently inconsistent and unpredictable. Locoregional therapies inducing immunogenic cell death, such as transarterial chemoembolization (TACE) or selective internal radiation therapy (SIRT), have the potential to act synergistically with immunotherapy. For the development of new approaches combining locoregional treatments with immunotherapy, a better understanding of the respective effects of TACE and SIRT on recruitment and activation of immune cells in HCC is needed. To address this question, we compared intra-tumor immune infiltrates in resected HCC after preoperative treatment with TACE or SIRT.
Data fromr patients undergoing partial hepatectomy for HCC, without preoperative treatment (SURG, n = 32), after preoperative TACE (TACE, n = 16), or preoperative SIRT (n = 12) were analyzed. Clinicopathological factors, tumor-infiltrating lymphocytes (TILs), CD4 and CD8 T cells, and granzyme B (GZB) expression in resected HCC, and postoperative overall and progression-free survival were compared between the three groups.
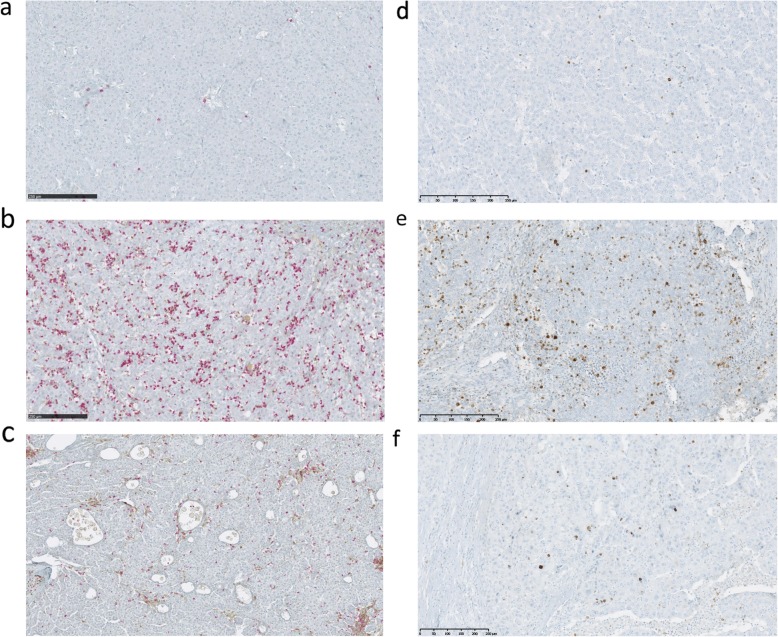
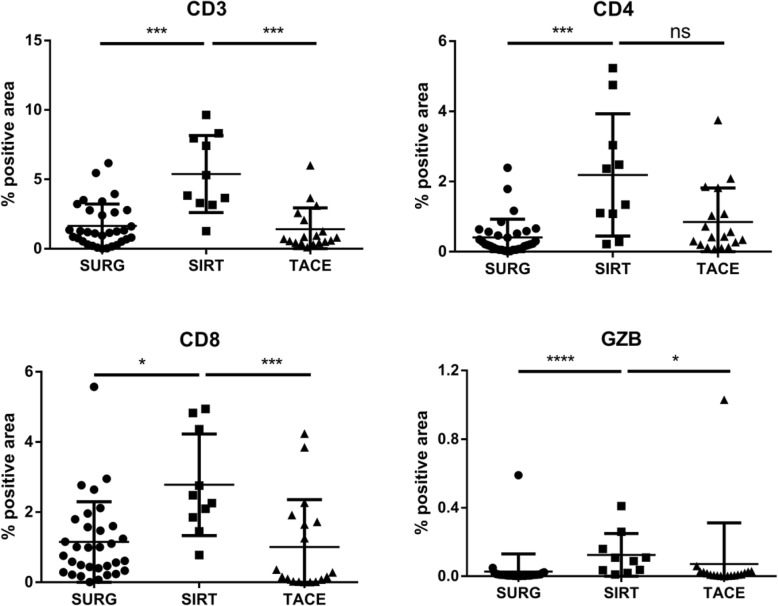
Clinicopathological and surgical characteristics were similar in the three groups. A significant increase in TILs, CD4 and CD8 T cells, and GZB expression was observed in resected HCC in SIRT as compared to TACE and SURG groups. No difference in immune infiltrates was observed between TACE and SURG patients. Within the SIRT group, the dose of irradiation affected the type of immune infiltrate. A significantly higher ratio of CD3 cells was observed in the peri-tumoral area in patients receiving < 100 Gy, whereas a higher ratio of intra-tumoral CD4 cells was observed in patients receiving > 100 Gy. Postoperative outcomes were similar in all groups. Irrespective of the preoperative treatment, the type and extent of immune infiltrates did not influence postoperative survival.
SIRT significantly promotes recruitment/activation of intra-tumor effector-type immune cells compared to TACE or no preoperative treatment. These results suggest that SIRT is a better candidate than TACE to be combined with immunotherapy for treatment of HCC. Evaluation of the optimal doses for SIRT for producing an immunogenic effect and the type of immunotherapy to be used require further evaluation in prospective studies.
免疫疗法为肝硬化患者的肝细胞癌(HCC)治疗提供了一种很有前途的选择,但目前其疗效并不一致且难以预测。诱导免疫原性细胞死亡的局部区域治疗,如经动脉化疗栓塞(TACE)或选择性内放射治疗(SIRT),有可能与免疫疗法协同作用。为了开发将局部区域治疗与免疫疗法相结合的新方法,需要更好地了解 TACE 和 SIRT 对 HCC 中免疫细胞募集和激活的各自影响。为了解决这个问题,我们比较了接受术前 TACE 或 SIRT 治疗后切除 HCC 中的肿瘤内免疫浸润。
分析了 32 例未行术前治疗(SURG)、16 例术前 TACE(TACE)和 12 例术前 SIRT(n=12)的 HCC 患者的部分肝切除术数据。比较三组患者的临床病理特征、肿瘤浸润淋巴细胞(TILs)、CD4 和 CD8 T 细胞、颗粒酶 B(GZB)在切除 HCC 中的表达以及术后总生存和无进展生存情况。
三组的临床病理和手术特征相似。与 TACE 和 SURG 组相比,SIRT 组在切除 HCC 中观察到 TILs、CD4 和 CD8 T 细胞以及 GZB 表达显著增加。TACE 和 SURG 患者的免疫浸润无差异。在 SIRT 组中,照射剂量影响免疫浸润的类型。接受<100Gy 照射的患者在肿瘤周围区域观察到 CD3 细胞的比例显著增加,而接受>100Gy 照射的患者在肿瘤内观察到 CD4 细胞的比例更高。所有组的术后结局相似。无论术前治疗如何,免疫浸润的类型和程度都不影响术后生存。
与 TACE 或无术前治疗相比,SIRT 可显著促进肿瘤内效应型免疫细胞的募集/激活。这些结果表明,SIRT 是与免疫疗法联合治疗 HCC 的更好选择。为了产生免疫原性作用,需要进一步评估 SIRT 的最佳剂量,以及要使用的免疫疗法类型,这需要在前瞻性研究中进行评估。