Clinical Research Division and.
Integrated Immunotherapy Research Center, Fred Hutchinson Cancer Research Center, Seattle, WA; and.
Blood. 2021 Jan 21;137(3):323-335. doi: 10.1182/blood.2020006770.
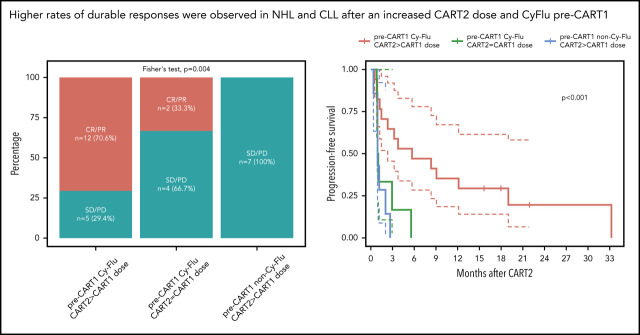
CD19-targeted chimeric antigen receptor-engineered (CD19 CAR) T-cell therapy has shown significant efficacy for relapsed or refractory (R/R) B-cell malignancies. Yet, CD19 CAR T cells fail to induce durable responses in most patients. Second infusions of CD19 CAR T cells (CART2) have been considered as a possible approach to improve outcomes. We analyzed data from 44 patients with R/R B-cell malignancies (acute lymphoblastic leukemia [ALL], n = 14; chronic lymphocytic leukemia [CLL], n = 9; non-Hodgkin lymphoma [NHL], n = 21) who received CART2 on a phase 1/2 trial (NCT01865617) at our institution. Despite a CART2 dose increase in 82% of patients, we observed a low incidence of severe toxicity after CART2 (grade ≥3 cytokine release syndrome, 9%; grade ≥3 neurotoxicity, 11%). After CART2, complete response (CR) was achieved in 22% of CLL, 19% of NHL, and 21% of ALL patients. The median durations of response after CART2 in CLL, NHL, and ALL patients were 33, 6, and 4 months, respectively. Addition of fludarabine to cyclophosphamide-based lymphodepletion before the first CAR T-cell infusion (CART1) and an increase in the CART2 dose compared with CART1 were independently associated with higher overall response rates and longer progression-free survival after CART2. We observed durable CAR T-cell persistence after CART2 in patients who received cyclophosphamide and fludarabine (Cy-Flu) lymphodepletion before CART1 and a higher CART2 compared with CART1 cell dose. The identification of 2 modifiable pretreatment factors independently associated with better outcomes after CART2 suggests strategies to improve in vivo CAR T-cell kinetics and responses after repeat CAR T-cell infusions, and has implications for the design of trials of novel CAR T-cell products after failure of prior CAR T-cell immunotherapies.
CD19 靶向嵌合抗原受体工程化 (CD19 CAR) T 细胞疗法已显示出对复发或难治性 (R/R) B 细胞恶性肿瘤的显著疗效。然而,CD19 CAR T 细胞在大多数患者中无法诱导持久反应。第二次输注 CD19 CAR T 细胞 (CART2) 已被认为是改善结果的一种可能方法。我们分析了在我们机构进行的一项 1/2 期试验 (NCT01865617) 中 44 例 R/R B 细胞恶性肿瘤 (急性淋巴细胞白血病 [ALL],n = 14;慢性淋巴细胞白血病 [CLL],n = 9;非霍奇金淋巴瘤 [NHL],n = 21) 患者接受 CART2 治疗的数据。尽管 82%的患者增加了 CART2 剂量,但我们观察到 CART2 后严重毒性的发生率较低 (≥3 级细胞因子释放综合征,9%;≥3 级神经毒性,11%)。在 CART2 后,CLL、NHL 和 ALL 患者的完全缓解 (CR) 率分别达到 22%、19%和 21%。CLL、NHL 和 ALL 患者在 CART2 后的中位反应持续时间分别为 33、6 和 4 个月。与 CART1 相比,在第一次 CAR T 细胞输注 (CART1) 前添加氟达拉滨和环磷酰胺的淋巴细胞耗竭以及增加 CART2 剂量与 CART2 后更高的总体反应率和更长的无进展生存期独立相关。我们观察到在接受 CART1 前接受环磷酰胺和氟达拉滨 (Cy-Flu) 淋巴细胞耗竭以及与 CART1 相比更高的 CART2 细胞剂量的患者中,在接受 CART2 后 CAR T 细胞具有持久的持久性。确定 2 个可修改的预处理因素与 CART2 后更好的结果独立相关,提示了在重复 CAR T 细胞输注后改善体内 CAR T 细胞动力学和反应的策略,并且对先前 CAR T 细胞免疫疗法失败后新型 CAR T 细胞产品试验的设计具有意义。