Clinical Division and Laboratory of Intensive Care Medicine, Department of Cellular and Molecular Medicine, KU Leuven, Herestraat 49, 3000, Leuven, Belgium.
Department of Medical and Surgical Specialties, Radiological Sciences and Public Health, University of Brescia, 25123, Brescia, Italy.
Intensive Care Med. 2020 Apr;46(4):637-653. doi: 10.1007/s00134-020-05944-4. Epub 2020 Feb 19.
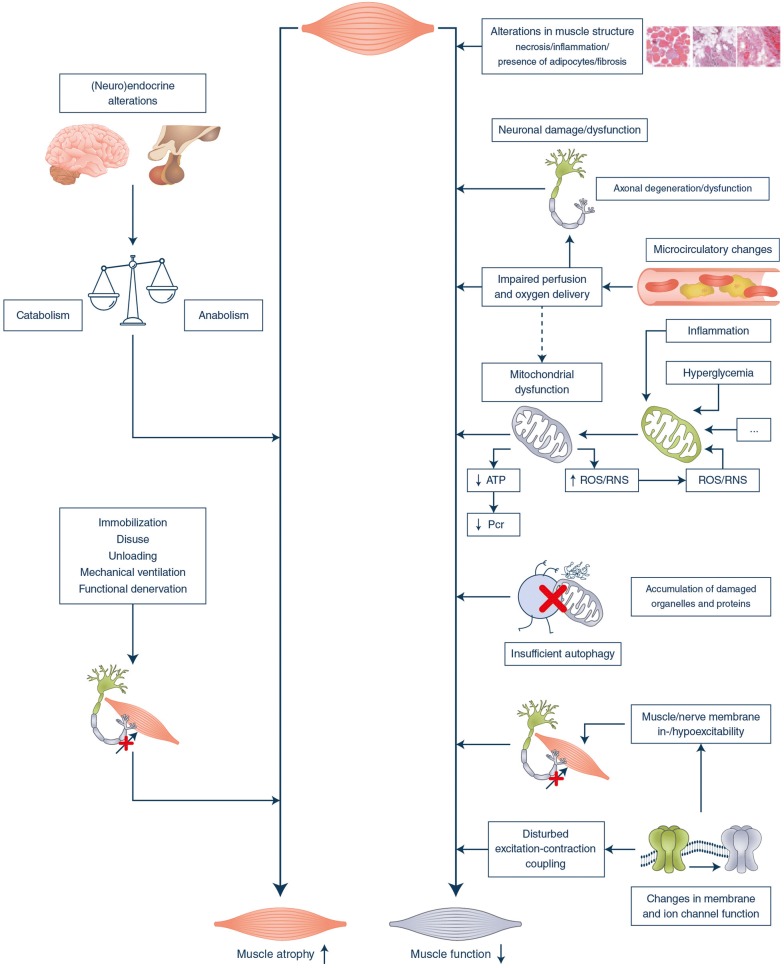
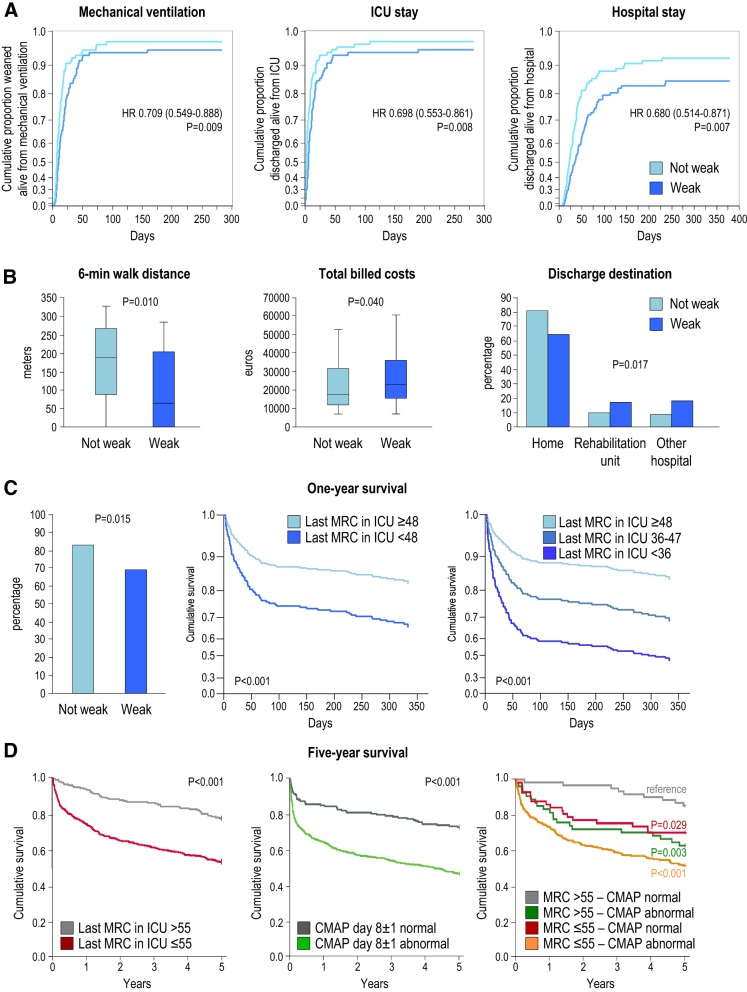
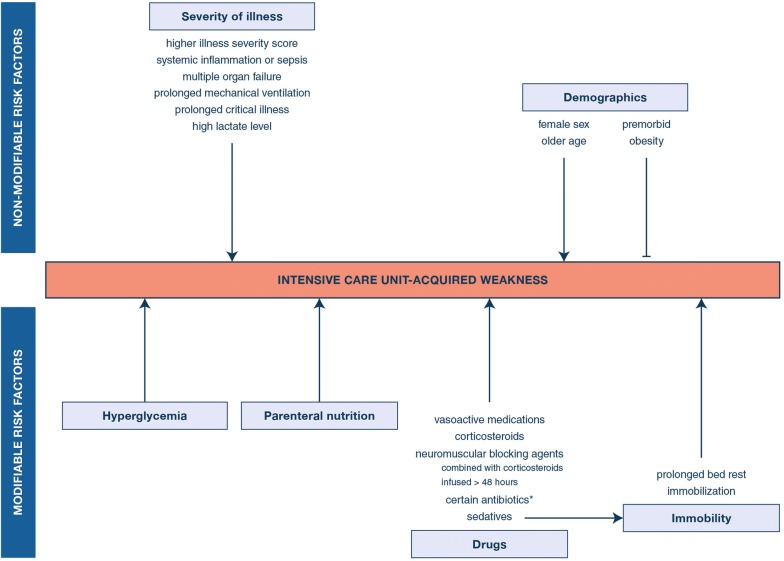
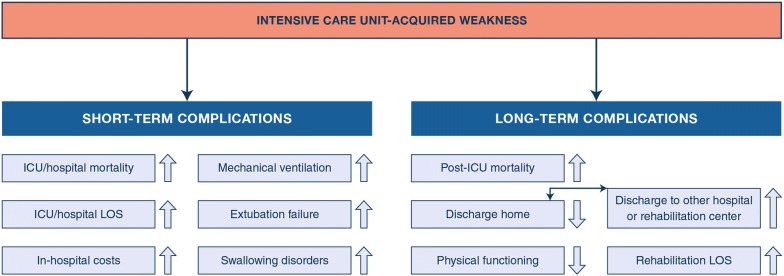
Critically ill patients often acquire neuropathy and/or myopathy labeled ICU-acquired weakness. The current insights into incidence, pathophysiology, diagnostic tools, risk factors, short- and long-term consequences and management of ICU-acquired weakness are narratively reviewed. PubMed was searched for combinations of "neuropathy", "myopathy", "neuromyopathy", or "weakness" with "critical illness", "critically ill", "ICU", "PICU", "sepsis" or "burn". ICU-acquired weakness affects limb and respiratory muscles with a widely varying prevalence depending on the study population. Pathophysiology remains incompletely understood but comprises complex structural/functional alterations within myofibers and neurons. Clinical and electrophysiological tools are used for diagnosis, each with advantages and limitations. Risk factors include age, weight, comorbidities, illness severity, organ failure, exposure to drugs negatively affecting myofibers and neurons, immobility and other intensive care-related factors. ICU-acquired weakness increases risk of in-ICU, in-hospital and long-term mortality, duration of mechanical ventilation and of hospitalization and augments healthcare-related costs, increases likelihood of prolonged care in rehabilitation centers and reduces physical function and quality of life in the long term. RCTs have shown preventive impact of avoiding hyperglycemia, of omitting early parenteral nutrition use and of minimizing sedation. Results of studies investigating the impact of early mobilization, neuromuscular electrical stimulation and of pharmacological interventions were inconsistent, with recent systematic reviews/meta-analyses revealing no or only low-quality evidence for benefit. ICU-acquired weakness predisposes to adverse short- and long-term outcomes. Only a few preventive, but no therapeutic, strategies exist. Further mechanistic research is needed to identify new targets for interventions to be tested in adequately powered RCTs.
危重病患者常发生神经病变和/或肌病,被称为 ICU 获得性肌无力。本文对 ICU 获得性肌无力的发病率、病理生理学、诊断工具、危险因素、短期和长期后果以及治疗进行了综述。通过 PubMed 检索了“神经病”、“肌病”、“神经肌肉病”或“肌无力”与“危重病”、“危重病”、“ICU”、“PICU”、“脓毒症”或“烧伤”的组合。ICU 获得性肌无力影响肢体和呼吸肌,其患病率因研究人群而异而存在广泛差异。病理生理学仍不完全清楚,但包括肌纤维和神经元内复杂的结构/功能改变。临床和电生理工具用于诊断,各有优缺点。危险因素包括年龄、体重、合并症、疾病严重程度、器官衰竭、接触可导致肌纤维和神经元功能障碍的药物、长期卧床和其他与重症监护相关的因素。ICU 获得性肌无力增加了 ICU 内、住院期间和长期死亡率、机械通气时间、住院时间以及医疗保健相关费用的风险,增加了在康复中心长期护理的可能性,并降低了长期的身体功能和生活质量。RCT 表明,避免高血糖、避免早期肠外营养和尽量减少镇静作用具有预防作用。早期运动、神经肌肉电刺激和药物干预研究的结果不一致,最近的系统评价/荟萃分析显示,获益的证据不足或只有低质量证据。ICU 获得性肌无力易导致短期和长期不良后果。目前仅有少数预防策略,但没有治疗策略。需要进一步的机制研究来确定新的干预靶点,以便在充分有力的 RCT 中进行测试。