Departments of Radiation Oncology, University of Miami Miller School of Medicine, Miami, Florida.
Departments of Radiation Oncology, University of Miami Miller School of Medicine, Miami, Florida.
Int J Radiat Oncol Biol Phys. 2020 Jun 1;107(2):305-315. doi: 10.1016/j.ijrobp.2020.01.052. Epub 2020 Feb 19.
A phase I clinical trial was designed to test the feasibility and toxicity of administering high-dose spatially fractionated radiation therapy to magnetic resonance imaging (MRI)-defined prostate tumor volumes, in addition to standard treatment.
We enrolled 25 men with favorable to high-risk prostate cancer and 1 to 3 suspicious multiparametric MRI (mpMRI) gross tumor volumes (GTVs). The mpMRI-GTVs were treated on day 1 with 12 to 14 Gy via dose cylinders using a lattice extreme ablative dose technique. The entire prostate, along with the proximal seminal vesicles, was then treated to 76 Gy at 2 Gy/fraction. For some high-risk patients, the distal seminal vesicles and pelvic lymph nodes received 56 Gy at 1.47 Gy/fraction concurrently in 38 fractions. The total dose to the lattice extreme ablative dose cylinder volume(s) was 88 to 90 Gy (112-123 Gy in 2.0 Gy equivalents, assuming an α-to-β ratio of 3).
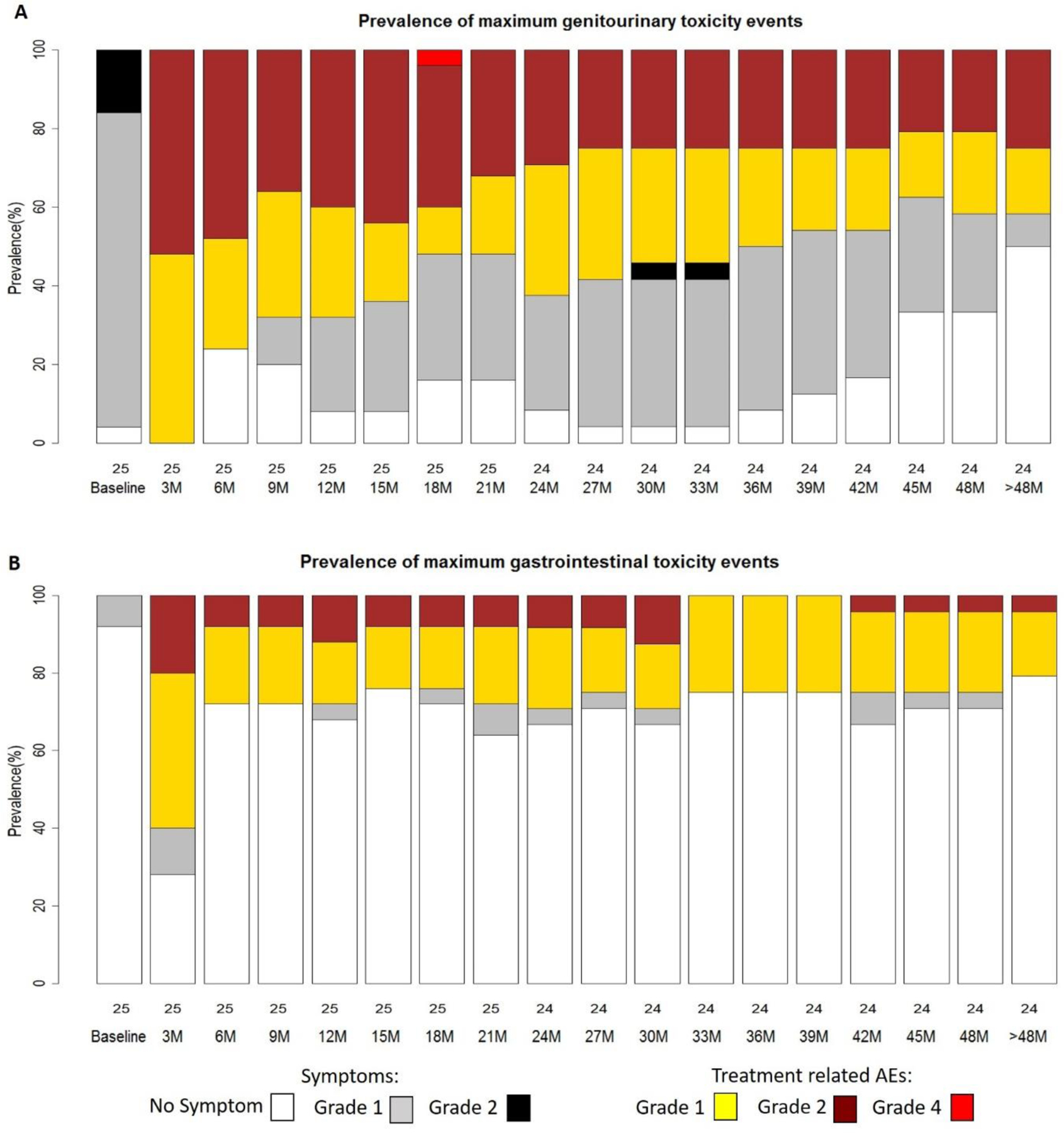
Dosimetric parameters were satisfactorily met. Median follow-up was 66 months. There were no grade 3 acute/subacute genitourinary or gastrointestinal adverse events. Maximum late genitourinary toxicity was grade 1 in 15 (60%), grade 2 in 4 (16%), and grade 4 in 1 (4%; sepsis after a posttreatment transurethral resection). Maximum late gastrointestinal toxicity was grade 1 in 11 (44%) and grade 2 in 4 (16%). Two patients experienced biochemical failure.
External beam radiation therapy delivered with an upfront spatially fractionated, stereotactic high-dose mpMRI-GTV boost is feasible and was not associated with any unexpected events. The technique is now part of a follow-up phase II randomized trial.
一项 I 期临床试验旨在测试对磁共振成像(MRI)定义的前列腺肿瘤体积进行高剂量空间分割放射治疗的可行性和毒性,此外还进行标准治疗。
我们招募了 25 名患有中高危前列腺癌和 1-3 个可疑多参数 MRI(mpMRI)大体肿瘤体积(GTV)的男性患者。mpMRI-GTVs 在第 1 天通过剂量筒使用晶格极消融剂量技术给予 12-14 Gy。然后,整个前列腺和近端精囊以 2 Gy/次的剂量给予 76 Gy。对于一些高危患者,远端精囊和骨盆淋巴结同时接受 56 Gy 的照射,共 38 次,每次 1.47 Gy。晶格极消融剂量筒体积的总剂量为 88-90 Gy(2.0 Gy 等效物为 112-123 Gy,假设α-β 比值为 3)。
剂量学参数得到了满意的满足。中位随访时间为 66 个月。无 3 级急性/亚急性泌尿生殖系统或胃肠道不良事件。晚期泌尿生殖系统毒性最大为 1 级 15 例(60%),2 级 4 例(16%),4 级 1 例(4%;治疗后经尿道前列腺切除术并发败血症)。晚期胃肠道毒性最大为 1 级 11 例(44%),2 级 4 例(16%)。有 2 例患者发生生化失败。
upfront 空间分割、立体定向高剂量 mpMRI-GTV 推量的外照射放射治疗是可行的,且没有任何意外事件发生。该技术现在是一项后续 II 期随机试验的一部分。