Center for Inflammatory Bowel Diseases, Department of General Surgery, Jinling Hospital, Medical School of Nanjing University, Nanjing, Jiangsu, China.
Department of Surgery, Surgical Professorial Unit, University Hospital Limerick, Limerick, Ireland.
Trials. 2020 Feb 21;21(1):210. doi: 10.1186/s13063-020-4105-x.
The structures of the mesentery including adipose tissue, nerves, and lymphatics play an important role in the pathogenesis and disease progression of Crohn's disease (CD). Conventional surgical resection for CD usually does not involve resecting the mesentery en bloc with the specimen. This contrasts with complete mesocolic excision (CME) in colorectal cancer, which involves radical resection of the mesentery. Preliminary evidence from smaller studies suggests that applying the principle of mesocolic excision to CD surgery may reduce the risk of postoperative recurrence. This randomized controlled trial is designed to test whether applying the principles of mesocolic excision to CD results in reduced postoperative recurrence. It also aims to evaluate intra- and postoperative morbidity between the two approaches.
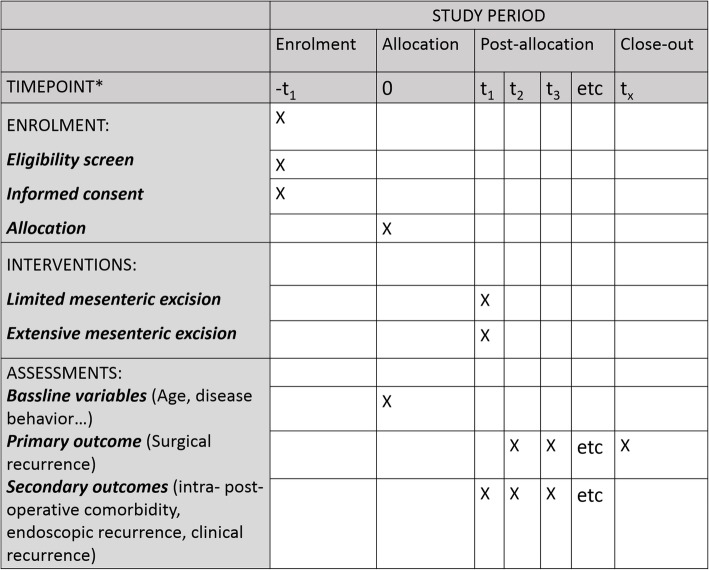
This international, multicenter, randomized controlled trial will randomize patients (n = 116) scheduled to undergo primary ileocolic resection to either receive extensive mesenteric excision (EME) or conventional ileocolic resection with limited mesenteric excision (LME). Five sites will recruit patients in three countries. In the EME group, the mesentery is resected following CME, while avoiding the root region, i.e., 1 cm from the root of the ileocolic artery and vein. In the LME group, the mesentery is retained, i.e., "close shave" or < 3 cm from the border of bowel. The primary end point will be surgical recurrence after surgery. The secondary end points will be the postoperative endoscopic and clinical recurrence, and intra- and postoperative morbidity. Demographics, risk factors, laboratory investigations, endoscopy, postoperative prophylaxis and imaging examination will be assessed. Analysis of the primary outcome will be on an intention-to-treat basis.
If mesocolic excision in CD reduces postoperative disease recurrence and does not increase morbidity, this trial has the potential to change practice and reduce recurrence of CD after surgical resection.
Clinical Trials.gov, ID: NCT03769922. Registered on February 27, 2019.
肠系膜的结构包括脂肪组织、神经和淋巴管,在克罗恩病(CD)的发病机制和疾病进展中起着重要作用。CD 的常规手术切除通常不涉及整块切除标本的肠系膜。这与结直肠癌的完整结肠系膜切除术(CME)形成对比,后者涉及肠系膜的根治性切除。来自较小研究的初步证据表明,将结肠系膜切除的原则应用于 CD 手术可能会降低术后复发的风险。本随机对照试验旨在测试将结肠系膜切除的原则应用于 CD 是否会降低术后复发率。它还旨在评估两种方法之间的围手术期发病率。
这项国际性、多中心、随机对照试验将对计划行原发性回结肠切除术的患者(n=116)进行随机分组,分别接受广泛肠系膜切除(EME)或有限肠系膜切除(LME)。三个国家的五个地点将招募患者。在 EME 组中,肠系膜按照 CME 进行切除,同时避免根部区域,即距回结肠动静脉根部 1cm。在 LME 组中,保留肠系膜,即“紧贴”或距肠边界<3cm。主要终点是手术后的手术复发。次要终点是术后内镜和临床复发以及围手术期发病率。将评估人口统计学、危险因素、实验室检查、内镜、术后预防和影像学检查。主要结局的分析将基于意向治疗。
如果 CD 中的结肠系膜切除可降低术后疾病复发率且不增加发病率,则该试验有可能改变实践并降低手术切除后 CD 的复发率。
ClinicalTrials.gov,ID:NCT03769922。于 2019 年 2 月 27 日注册。