Massachusetts General Hospital Cancer Center and Department of Medicine, Massachusetts General Hospital, Boston, Massachusetts.
Harvard Medical School, Boston, Massachusetts.
Clin Cancer Res. 2020 Jun 1;26(11):2535-2545. doi: 10.1158/1078-0432.CCR-19-3906. Epub 2020 Feb 21.
Most -positive lung cancers will develop ALK-independent resistance after treatment with next-generation ALK inhibitors. amplification has been described in patients progressing on ALK inhibitors, but frequency of this event has not been comprehensively assessed.
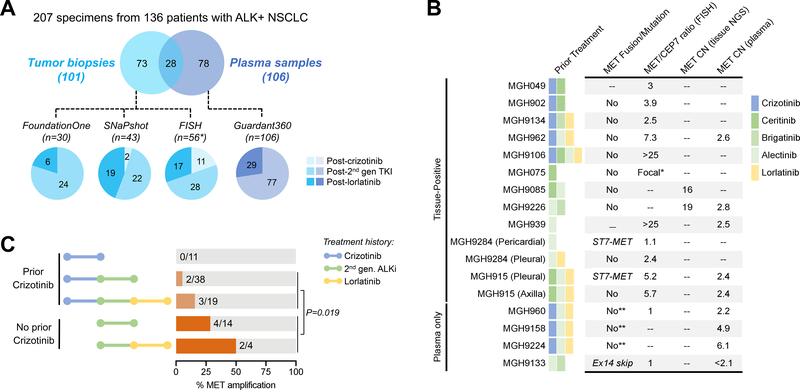
We performed FISH and/or next-generation sequencing on 207 posttreatment tissue ( = 101) or plasma ( = 106) specimens from patients with ALK-positive lung cancer to detect genetic alterations. We evaluated ALK inhibitor sensitivity in cell lines with alterations and assessed antitumor activity of ALK/MET blockade in ALK-positive cell lines and 2 patients with MET-driven resistance.
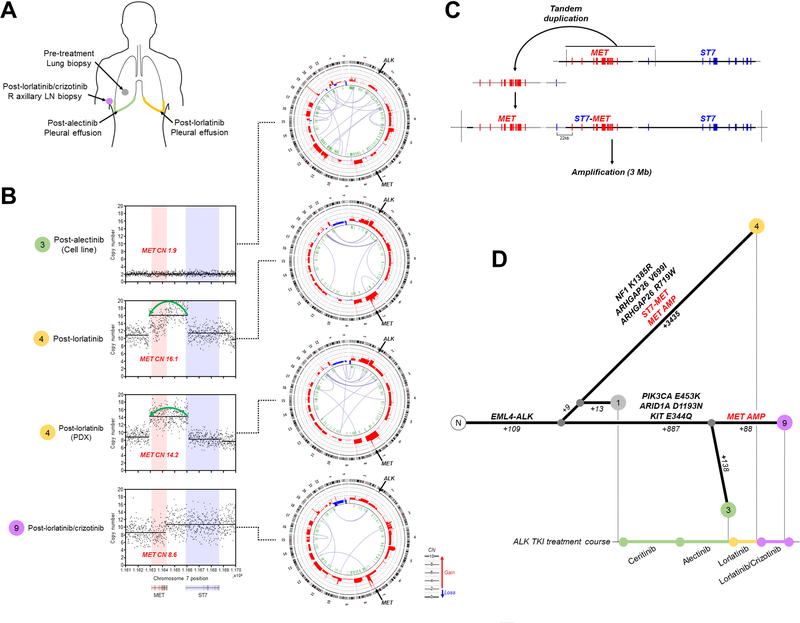
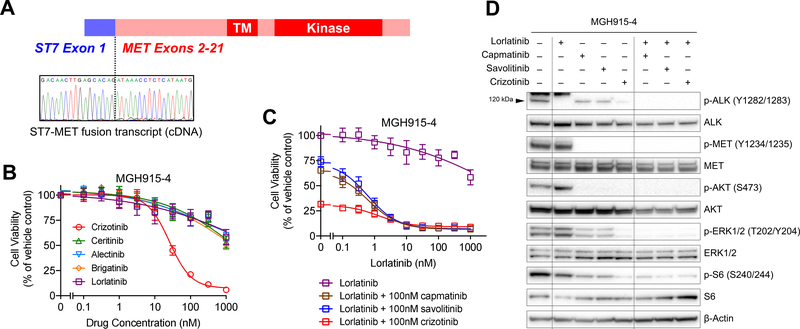
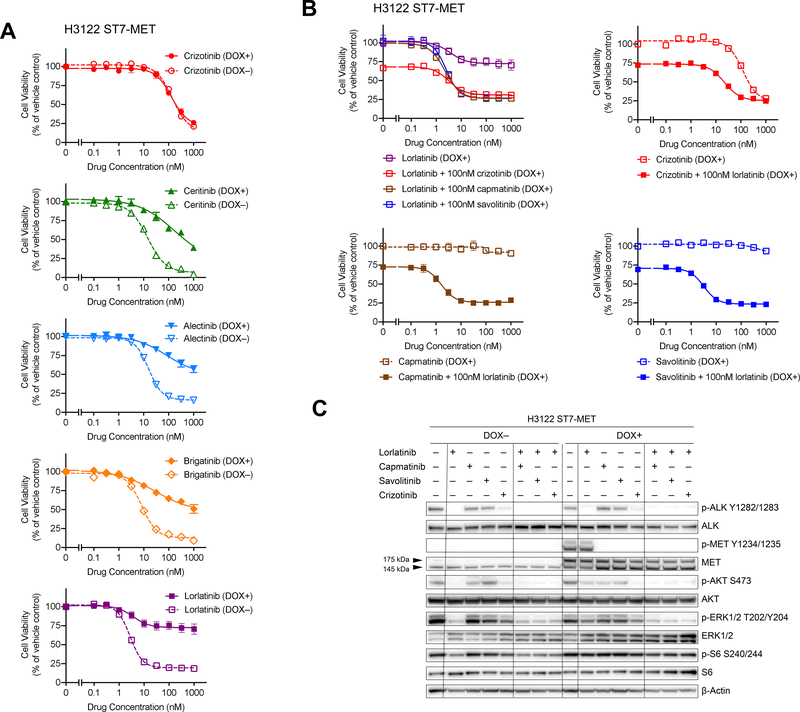
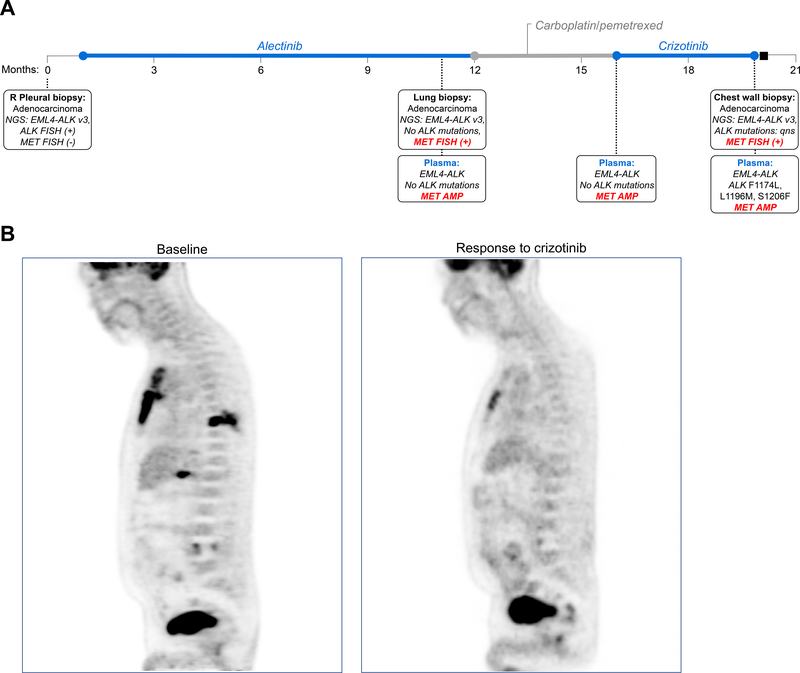
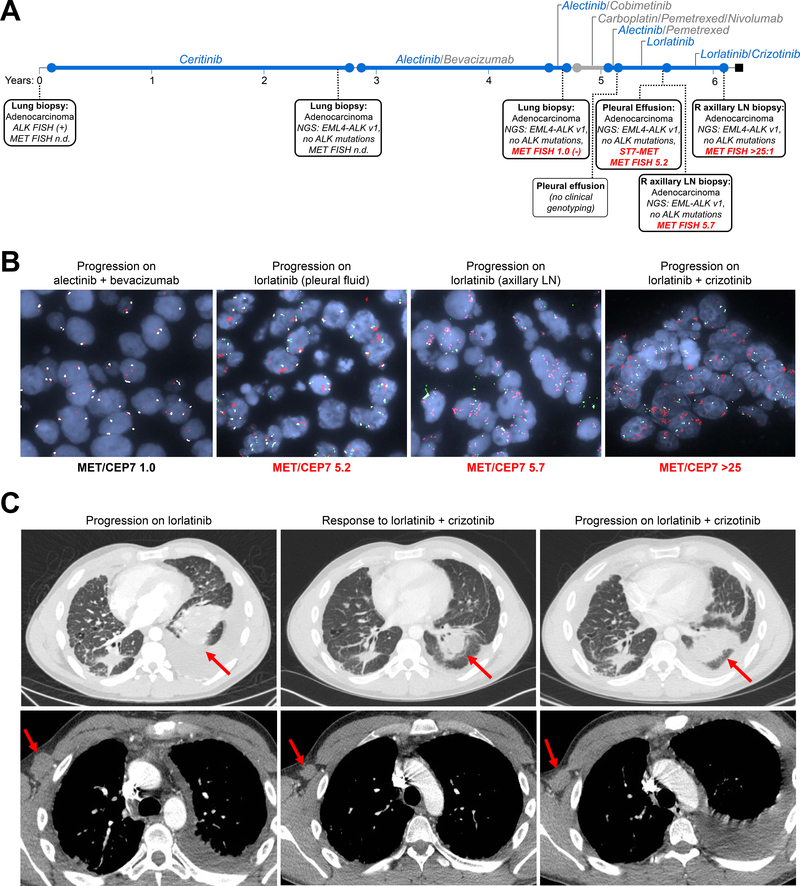
amplification was detected in 15% of tumor biopsies from patients relapsing on next-generation ALK inhibitors, including 12% and 22% of biopsies from patients progressing on second-generation inhibitors or lorlatinib, respectively. Patients treated with a second-generation ALK inhibitor in the first-line setting were more likely to develop amplification than those who had received next-generation ALK inhibitors after crizotinib ( = 0.019). Two tumor specimens harbored an identical rearrangement, one of which had concurrent amplification. Expressing in the sensitive H3122 ALK-positive cell line induced resistance to ALK inhibitors that was reversed with dual ALK/MET inhibition. MET inhibition resensitized a patient-derived cell line harboring both and amplification to ALK inhibitors. Two patients with ALK-positive lung cancer and acquired alterations achieved rapid responses to ALK/MET combination therapy.
Treatment with next-generation ALK inhibitors, particularly in the first-line setting, may lead to MET-driven resistance. Patients with acquired alterations may derive clinical benefit from therapies that target both ALK and MET.
大多数阳性肺癌患者在接受下一代 ALK 抑制剂治疗后会出现 ALK 非依赖性耐药。在接受 ALK 抑制剂治疗后进展的患者中已经描述了扩增,但尚未全面评估该事件的频率。
我们对 207 个治疗后组织(n=101)或血浆(n=106)标本进行了 FISH 和/或下一代测序,以检测遗传改变。我们评估了具有改变的细胞系中 ALK 抑制剂的敏感性,并评估了 ALK/MET 阻断在 ALK 阳性细胞系和 2 名 MET 驱动耐药患者中的抗肿瘤活性。
在接受下一代 ALK 抑制剂治疗后复发的患者的肿瘤活检中,检测到扩增,包括分别接受第二代抑制剂或洛拉替尼治疗的患者中 12%和 22%的活检。在一线治疗中接受第二代 ALK 抑制剂治疗的患者比接受克唑替尼后接受下一代 ALK 抑制剂治疗的患者更有可能发展为扩增(=0.019)。两个肿瘤标本均存在相同的重排,其中一个伴有扩增。在敏感的 H3122 ALK 阳性细胞系中表达,诱导对 ALK 抑制剂的耐药,而双重 ALK/MET 抑制可逆转耐药。MET 抑制使同时存在和扩增的患者来源细胞系对 ALK 抑制剂重新敏感。两名患有阳性肺癌且获得改变的患者对 ALK/MET 联合治疗迅速产生反应。
接受下一代 ALK 抑制剂治疗,特别是在一线治疗中,可能导致 MET 驱动的耐药。获得改变的患者可能从靶向 ALK 和 MET 的治疗中获得临床益处。