Zhang Xue-Lian, Wan Gang, Yuan Ming-Xia, Yang Guang-Ran, Fu Han-Jing, Zhu Liang-Xiang, Xie Rong-Rong, Lv Yu-Jie, Zhang Jian-Dong, Li Yu-Ling, Dai Qin-Fang, Ji Yu, Holman Rury R, Yuan Shen-Yuan
Department of Endocrinology, Beijing Tongren Hospital, Capital Medical University, Beijing, China.
Medical records and Statistics Department, Beijing Ditan Hospital, Capital Medical University, Beijing, China.
Diabetes Ther. 2020 Apr;11(4):885-903. doi: 10.1007/s13300-020-00782-5. Epub 2020 Feb 21.
To date, research is lacking on the development of a cardiovascular disease (CVD) risk assessment tool for people with diabetes mellitus, in general, and for Chinese patients with diabetes in particular. We have explored CVD risk assessment tools for Chinese patients with diabetes. Here, we report our investigation of cardiovascular risk assessment using the improved Framingham Risk Score (I-FRS) in patients with type 2 diabetes mellitus (T2DM) in Beijing communities.
A total of 3232 patients with T2DM attending Beijing community health centers were enrolled in this study. FRS were used to predict CVD risk in all patients at baseline using the following risk scores for glycated hemoglobin (HbA1c) categories: 0 = HbA1c ≤ 7.0%; 1 = 7.0% < HbA1c ≤ 7.9%; 2 = 8.0% < HbA1c ≤ 8.9%; and 3 = HbA1c > 9.0%. The I-FRS was use to stratify all patients into low (I-FRS < 10%), medium (I-FRS 10-20%), and high (I-FRS > 20%) FRS strata. All treatments administered in the Beijing Communities Diabetes Study were in accordance with national guidelines for T2DM in China, and patients regularly attended clinical consultations with professors in endocrinology, who were experts in their respective speciality, from top tier hospitals. After 10 years, patients were followed-up to assess the long-term effects of the multifactorial interventions. Statistical analysis was performed using SAS® software (SAS Institute, Inc., Cary, NC, USA).
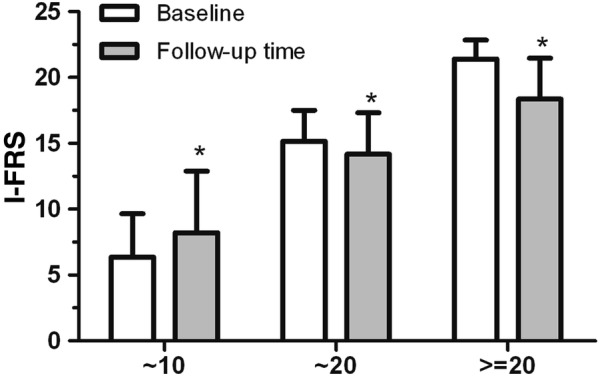
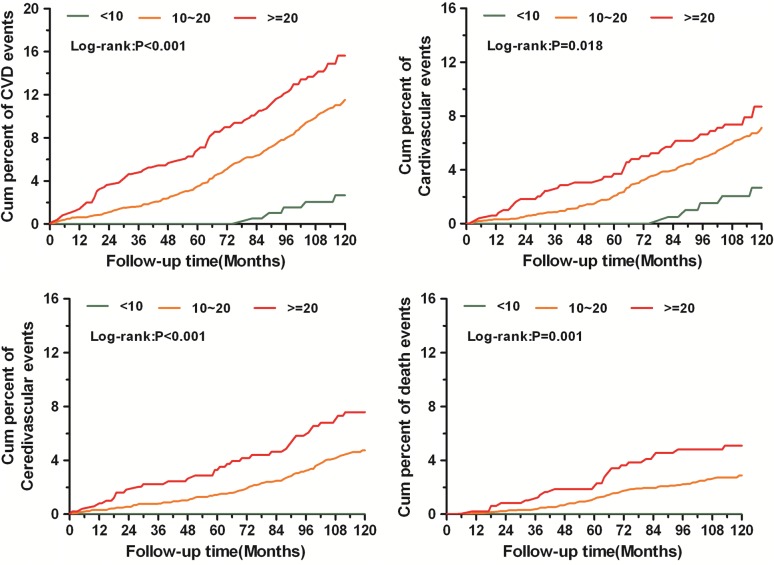
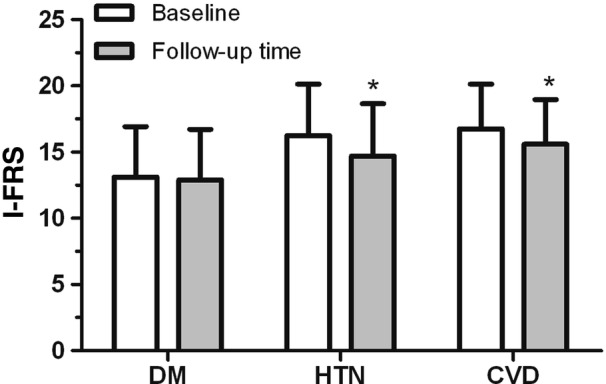
The receiver operating characteristic curve of the I-FRS showed significant prediction accuracy for the actual incidence of CVD events. At baseline, subjects in the high FRS stratum for diabetes were more prone to be elderly and to have a longer duration of T2DM, higher systolic blood pressure, and higher lipid profiles. Subjects in the medium and high FRS strata had a higher incidence of CVD events than those in the no-complications group (DM group with no blood pressure issues) (P < 0.001). The 10-year hazard ratios for CVD events in diabetic patients with I-FRS score > 20% was 12.5-fold higher than that of patients with I-FRS score < 10%. Multifactorial intervention significantly reduced the I-FRS of the three FRS strata in patients with T2DM. The post-intervention I-FRS for the hypertension and CVD groups of patients were significantly lower than the respective baseline I-FRS. Cox multivariate analyses revealed that patients in the medium and high FRS strata had higher incidences of endpoint events than those in the low FRS stratum.
The I-FRS plays an important role in predicting CVD in patients with T2DM. Multifactorial interventions for CVD risk factors over 10-year follow-up lowered the estimated 10-year risk for CVD events in persons with diabetes. We suggest the use of the I-FRS score to stratify a patient's risk of CVD when analyzing the efficacy of diabetes management. Aggressive risk reduction should be focused on those individuals with a high I-FRS score.
ChiCTR-TRC-13003978 and ChiCTR-OOC-15006090.
迄今为止,总体上缺乏针对糖尿病患者,尤其是中国糖尿病患者的心血管疾病(CVD)风险评估工具的研究。我们探索了适用于中国糖尿病患者的CVD风险评估工具。在此,我们报告在北京社区2型糖尿病(T2DM)患者中使用改良的弗明汉风险评分(I-FRS)进行心血管风险评估的调查结果。
本研究纳入了3232名在北京社区卫生中心就诊的T2DM患者。使用FRS在基线时根据糖化血红蛋白(HbA1c)类别对应的以下风险评分预测所有患者的CVD风险:0 = HbA1c≤7.0%;1 = 7.0%<HbA1c≤7.9%;2 = 8.0%<HbA1c≤8.9%;3 = HbA1c>9.0%。使用I-FRS将所有患者分为低(I-FRS<10%)、中(I-FRS 10-20%)和高(I-FRS>20%)FRS分层。北京社区糖尿病研究中给予的所有治疗均符合中国T2DM的国家指南,患者定期到顶级医院内分泌科教授处进行临床会诊,这些教授是各自领域的专家。10年后,对患者进行随访以评估多因素干预的长期效果。使用SAS®软件(美国北卡罗来纳州卡里市SAS研究所)进行统计分析。
I-FRS的受试者工作特征曲线显示对CVD事件的实际发生率具有显著的预测准确性。在基线时,糖尿病高FRS分层的受试者更倾向于年龄较大、T2DM病程较长、收缩压较高和血脂水平较高。中、高FRS分层的受试者CVD事件发生率高于无并发症组(无血压问题的糖尿病组)(P<0.001)。I-FRS评分>20%的糖尿病患者发生CVD事件的10年风险比I-FRS评分<10%的患者高12.5倍。多因素干预显著降低了T2DM患者三个FRS分层的I-FRS。高血压和CVD组患者干预后的I-FRS显著低于各自的基线I-FRS。Cox多变量分析显示,中、高FRS分层的患者终点事件发生率高于低FRS分层的患者。
I-FRS在预测T2DM患者的CVD方面发挥着重要作用。在10年的随访中对CVD危险因素进行多因素干预降低了糖尿病患者发生CVD事件的估计10年风险。我们建议在分析糖尿病管理效果时使用I-FRS评分对患者的CVD风险进行分层。应将积极的风险降低重点放在I-FRS评分高的个体上。
ChiCTR-TRC-13003978和ChiCTR-OOC-15006090。