Shahn Zach, Shapiro Nathan I, Tyler Patrick D, Talmor Daniel, Lehman Li-Wei H
IBM Research, Yorktown Heights, NY, USA.
MIT-IBM Watson AI Lab, Cambridge, USA.
Crit Care. 2020 Feb 22;24(1):62. doi: 10.1186/s13054-020-2767-0.
In septic patients, multiple retrospective studies show an association between large volumes of fluids administered in the first 24 h and mortality, suggesting a benefit to fluid restrictive strategies. However, these studies do not directly estimate the causal effects of fluid-restrictive strategies, nor do their analyses properly adjust for time-varying confounding by indication. In this study, we used causal inference techniques to estimate mortality outcomes that would result from imposing a range of arbitrary limits ("caps") on fluid volume administration during the first 24 h of intensive care unit (ICU) care.
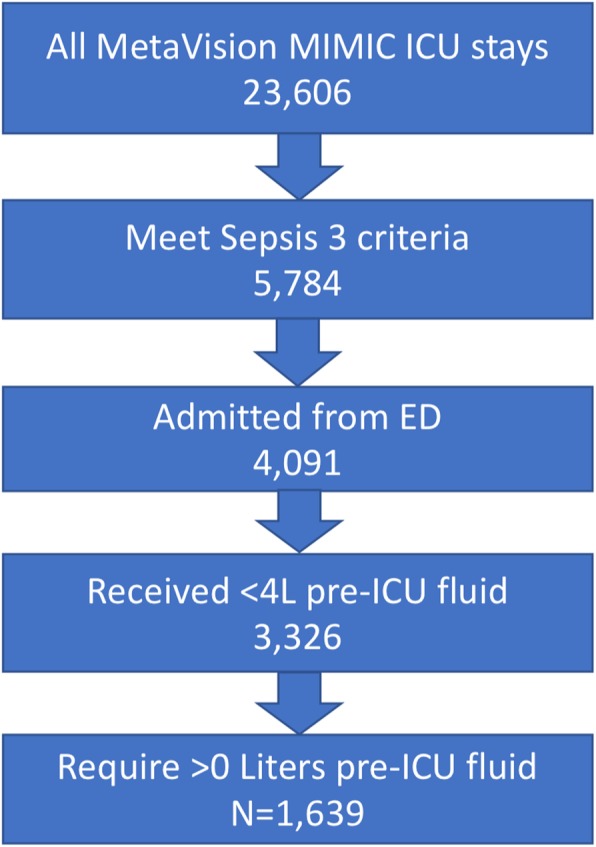
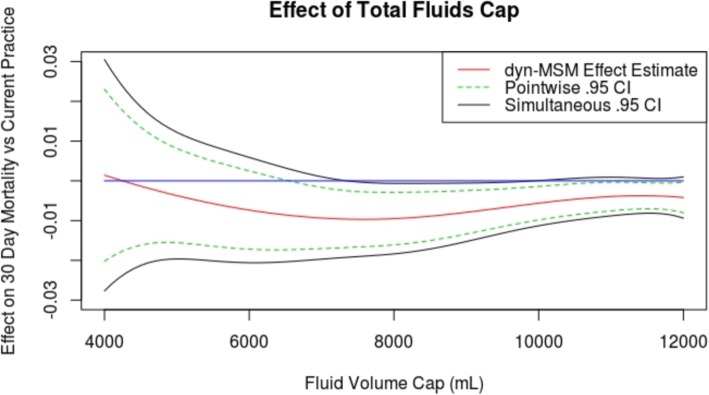
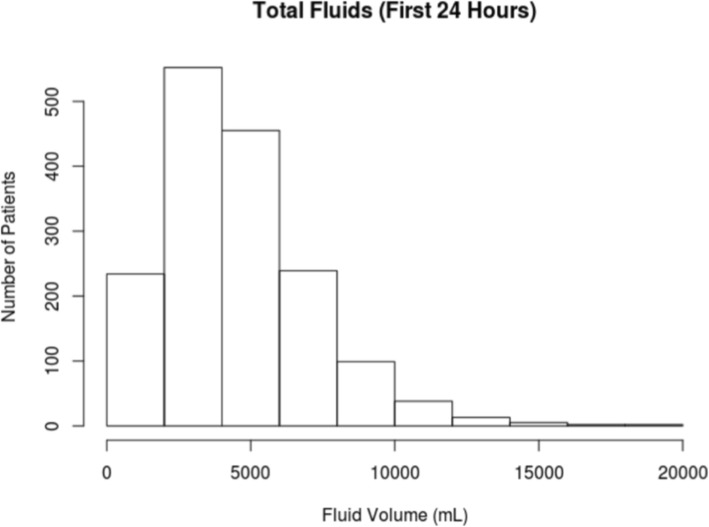
Retrospective cohort study SETTING: ICUs at the Beth Israel Deaconess Medical Center, 2008-2012 PATIENTS: One thousand six hundred thirty-nine septic patients (defined by Sepsis-3 criteria) 18 years and older, admitted to the ICU from the emergency department (ED), who received less than 4 L fluids administered prior to ICU admission MEASUREMENTS AND MAIN RESULTS: Data were obtained from the Medical Information Mart for Intensive Care III (MIMIC-III). We employed a dynamic Marginal Structural Model fit by inverse probability of treatment weighting to obtain confounding adjusted estimates of mortality rates that would have been observed had fluid resuscitation volume caps between 4 L-12 L been imposed on the population. The 30-day mortality in our cohort was 17%. We estimated that caps between 6 and 10 L on 24 h fluid volume would have reduced 30-day mortality by - 0.6 to - 1.0%, with the greatest reduction at 8 L (- 1.0% mortality, 95% CI [- 1.6%, - 0.3%]).
We found that 30-day mortality would have likely decreased relative to observed mortality under current practice if these patients had been subject to "caps" on the total volume of fluid administered between 6 and 10 L, with the greatest reduction in mortality rate at 8 L.
在脓毒症患者中,多项回顾性研究表明,在最初24小时内大量补液与死亡率之间存在关联,这表明采用液体限制策略可能有益。然而,这些研究并未直接估计液体限制策略的因果效应,其分析也未针对因适应证导致的随时间变化的混杂因素进行恰当调整。在本研究中,我们使用因果推断技术来估计在重症监护病房(ICU)治疗的最初24小时内对液体输入量施加一系列任意限制(“上限”)所导致的死亡结局。
回顾性队列研究
2008 - 2012年贝斯以色列女执事医疗中心的ICU
1639例脓毒症患者(根据脓毒症-3标准定义),年龄18岁及以上,从急诊科(ED)收入ICU,在ICU入院前接受的补液量少于4升
数据来自重症监护医学信息集市III(MIMIC-III)。我们采用逆概率加权法拟合动态边际结构模型,以获得如果对人群施加4升 - 12升的液体复苏量上限时可能观察到的死亡率的混杂因素调整估计值。我们队列中的30天死亡率为17%。我们估计,24小时液体量上限在6升至10升之间可使30天死亡率降低 - 0.6%至 - 1.0%。在8升时降低幅度最大(死亡率为 - 1.0%,95%置信区间[- 1.6%, - 0.3%])。
我们发现,如果这些患者在6升至10升的液体输入总量上受到“上限”限制,相对于当前实践中观察到的死亡率,30天死亡率可能会降低,在8升时死亡率降低幅度最大。