Department of Rehabilitation Research, University of Potsdam, Germany.
Institute of Medical Biometry and Informatics (IMBI), University of Heidelberg, Germany.
Eur J Prev Cardiol. 2020 Nov;27(16):1756-1774. doi: 10.1177/2047487320905719. Epub 2020 Feb 23.
Despite numerous studies and meta-analyses the prognostic effect of cardiac rehabilitation is still under debate. This update of the Cardiac Rehabilitation Outcome Study (CROS II) provides a contemporary and practice focused approach including only cardiac rehabilitation interventions based on published standards and core components to evaluate cardiac rehabilitation delivery and effectiveness in improving patient prognosis.
A systematic review and meta-analysis.
Randomised controlled trials and retrospective and prospective controlled cohort studies evaluating patients after acute coronary syndrome, coronary artery bypass grafting or mixed populations with coronary artery disease published until September 2018 were included.
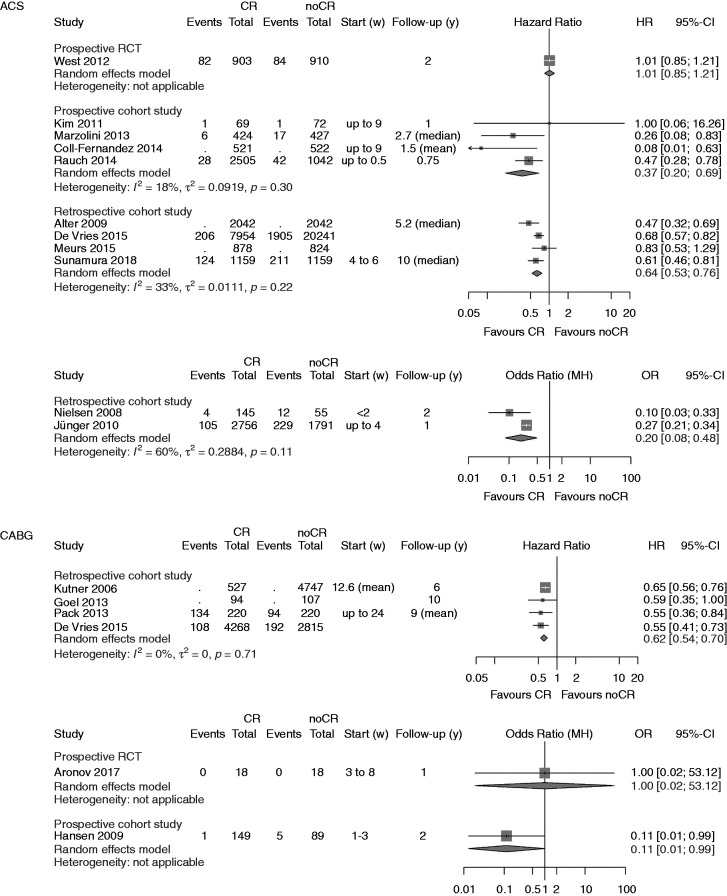
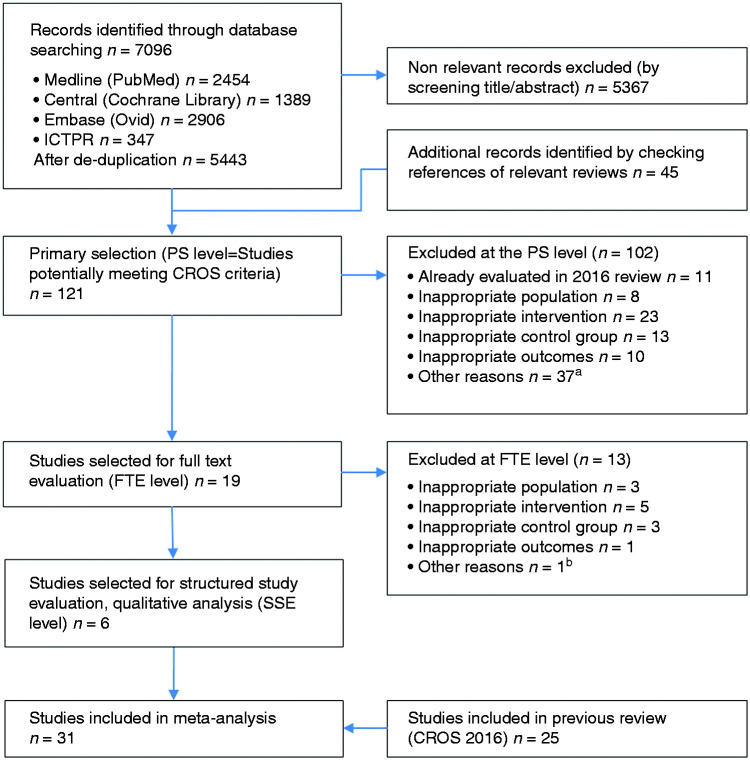
Based on CROS inclusion criteria out of 7096 abstracts six additional studies including 8671 patients were identified (two randomised controlled trials, two retrospective controlled cohort studies, two prospective controlled cohort studies). In total, 31 studies including 228,337 patients were available for this meta-analysis (three randomised controlled trials, nine prospective controlled cohort studies, 19 retrospective controlled cohort studies; 50,653 patients after acute coronary syndrome 14,583, after coronary artery bypass grafting 163,101, mixed coronary artery disease populations; follow-up periods ranging from 9 months to 14 years). Heterogeneity in design, cardiac rehabilitation delivery, biometrical assessment and potential confounders was considerable. Controlled cohort studies showed a significantly reduced total mortality (primary endpoint) after cardiac rehabilitation participation in patients after acute coronary syndrome (prospective controlled cohort studies: hazard ratio (HR) 0.37, 95% confidence interval (CI) 0.20-0.69; retrospective controlled cohort studies HR 0.64, 95% CI 0.53-0.76; prospective controlled cohort studies odds ratio 0.20, 95% CI 0.08-0.48), but the single randomised controlled trial fulfilling the CROS inclusion criteria showed neutral results. Cardiac rehabilitation participation was also associated with reduced total mortality in patients after coronary artery bypass grafting (retrospective controlled cohort studies HR 0.62, 95% CI 0.54-0.70, one single randomised controlled trial without fatal events), and in mixed coronary artery disease populations (retrospective controlled cohort studies HR 0.52, 95% CI 0.36-0.77; two out of 10 controlled cohort studies with neutral results).
CROS II confirms the effectiveness of cardiac rehabilitation participation after acute coronary syndrome and after coronary artery bypass grafting in actual clinical practice by reducing total mortality under the conditions of current evidence-based coronary artery disease treatment. The data of CROS II, however, underscore the urgent need to define internationally accepted minimal standards for cardiac rehabilitation delivery as well as for scientific evaluation.
尽管有大量的研究和荟萃分析,但心脏康复的预后效果仍存在争议。本项心脏康复结果研究(CROS II)的更新提供了一种现代且注重实践的方法,仅纳入基于已发表标准和核心内容的心脏康复干预措施,以评估心脏康复的实施情况及其改善患者预后的效果。
系统评价和荟萃分析。
纳入直至 2018 年 9 月发表的急性冠状动脉综合征、冠状动脉旁路移植术或混合冠心病患者的随机对照试验和回顾性及前瞻性对照队列研究。
基于 CROS 的纳入标准,从 7096 篇摘要中确定了另外 6 项研究,共纳入 8671 例患者(2 项随机对照试验、2 项回顾性对照队列研究、2 项前瞻性对照队列研究)。总共 31 项研究(3 项随机对照试验、9 项前瞻性对照队列研究、19 项回顾性对照队列研究),共 228337 例患者纳入本项荟萃分析(急性冠状动脉综合征后 50653 例患者,冠状动脉旁路移植术后 14583 例患者,混合冠心病患者 163101 例患者;随访时间 9 个月至 14 年)。在设计、心脏康复实施、生物统计学评估和潜在混杂因素方面存在显著的异质性。对照队列研究显示,急性冠状动脉综合征后接受心脏康复治疗的患者全因死亡率(主要终点)显著降低(前瞻性对照队列研究:风险比(HR)0.37,95%置信区间(CI)0.20-0.69;回顾性对照队列研究 HR 0.64,95%CI 0.53-0.76;前瞻性对照队列研究比值比 0.20,95%CI 0.08-0.48),但符合 CROS 纳入标准的唯一随机对照试验结果为中性。心脏康复治疗也与冠状动脉旁路移植术后患者(回顾性对照队列研究 HR 0.62,95%CI 0.54-0.70,1 项随机对照试验无死亡事件)和混合冠心病患者(回顾性对照队列研究 HR 0.52,95%CI 0.36-0.77;10 项对照队列研究中有 2 项结果为中性)的全因死亡率降低相关。
CROS II 通过降低当前循证治疗冠心病条件下的全因死亡率,证实了急性冠状动脉综合征和冠状动脉旁路移植术后心脏康复治疗的有效性。CROS II 的数据突出表明,迫切需要为心脏康复治疗提供以及科学评估制定国际公认的最低标准。