Department of Anaesthesiology and Pain Medicine Inselspital Bern University Hospital University of Bern Switzerland.
Department of Diagnostic, Interventional and Paediatric Radiology Inselspital Bern University Hospital University of Bern Switzerland.
J Am Heart Assoc. 2020 Mar 3;9(5):e014739. doi: 10.1161/JAHA.119.014739. Epub 2020 Feb 22.
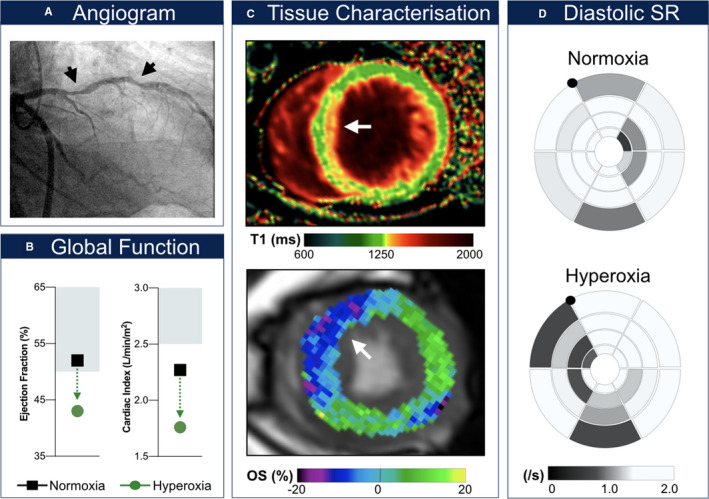
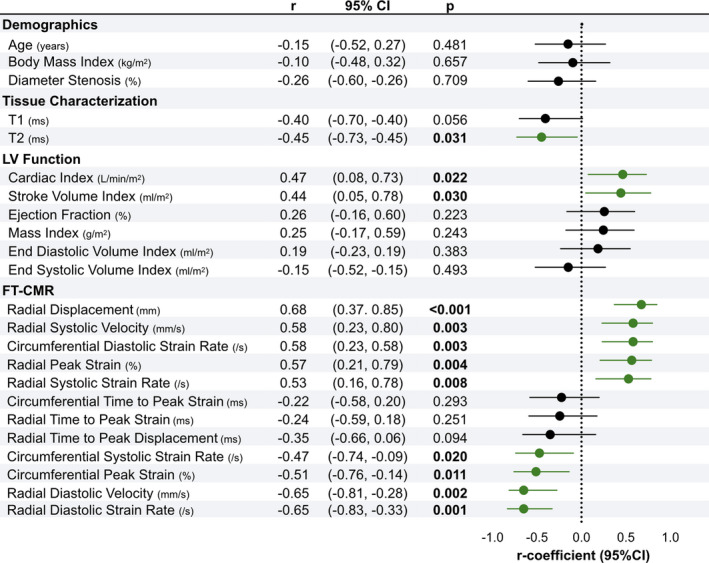
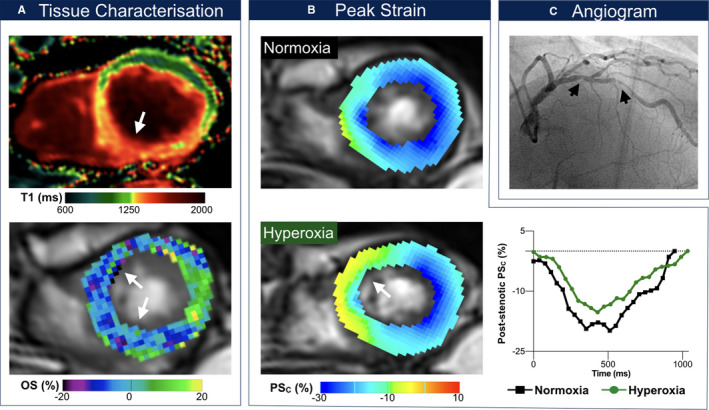
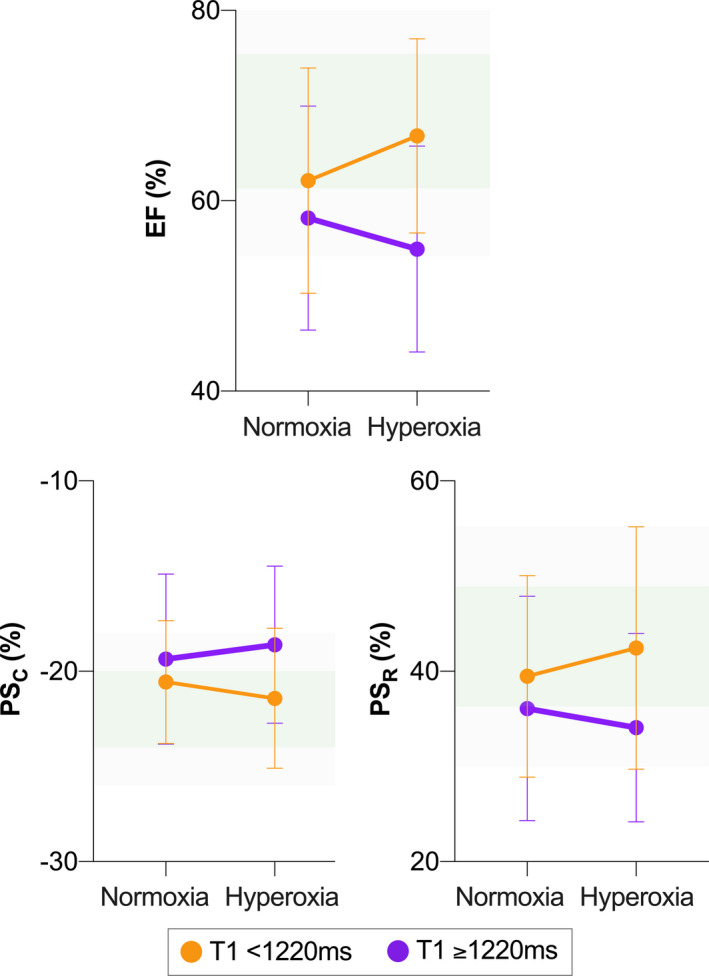
Background The impact of hyperoxia, that is, supraphysiological arterial partial pressure of O, on myocardial oxygen balance and function in stable multivessel coronary artery disease (CAD) is poorly understood. In this observational study, we assessed myocardial effects of inhalational hyperoxia in patients with CAD using a comprehensive cardiovascular magnetic resonance exam. Methods and Results Twenty-five patients with stable CAD underwent a contrast-free cardiovascular magnetic resonance exam in the interval between their index coronary angiography and subsequent revascularization. The cardiovascular magnetic resonance exam involved T1 and T2 mapping for tissue characterization (fibrosis, edema) as well as function imaging, from which strain analysis was derived, and oxygenation-sensitive cardiovascular magnetic resonance imaging. The latter modalities were both acquired at room air and after breathing pure O by face mask at 10 L/min for 5 minutes. In 14 of the 25 CAD patients (56%), hyperoxia induced poststenotic myocardial deoxygenation with a subsequent oxygenation discordance across the myocardium. Extent of deoxygenation was correlated to degree of stenosis (=-0.434, =0.033). Hyperoxia-associated poststenotic deoxygenation was accompanied by ipsiregional reduction of diastolic strain rate (1.39±0.57 versus 1.18±0.65; =0.045) and systolic radial velocity (37.40±17.22 versus 32.88±13.58; =0.038). Increased T2, as well as lower cardiac index, and defined abnormal strain parameters on room air were predictive for hyperoxia-induced abnormalities (<0.05). Furthermore, in patients with prolonged native T1 (>1220 ms), hyperoxia reduced ejection fraction and peak strain. Conclusions Patients with CAD and pre-existent myocardial injury who respond to hyperoxic challenge with strain abnormalities appear susceptible for hyperoxia-induced regional deoxygenation and deterioration of myocardial function. Clinical Trial Registration URL: http://www.clinicaltrials.gov. Unique identifier: NCT02233634.
高氧血症,即动脉氧分压高于生理范围,对稳定多支冠状动脉疾病(CAD)患者的心肌氧平衡和功能的影响知之甚少。在这项观察性研究中,我们使用综合心血管磁共振检查评估了 CAD 患者吸入高氧对心肌的影响。
25 例稳定 CAD 患者在其指数冠状动脉造影和随后的血运重建之间接受了无对比剂心血管磁共振检查。心血管磁共振检查包括 T1 和 T2 映射以进行组织特征(纤维化、水肿)以及功能成像,从中得出应变分析,以及氧敏感的心血管磁共振成像。后者在室温和通过面罩呼吸 10 L/min 的纯 O 5 分钟后,分别在室温和呼吸纯 O 后获得。在 25 例 CAD 患者中的 14 例(56%)中,高氧诱导了后狭窄心肌去氧,随后心肌出现氧合不匹配。去氧程度与狭窄程度相关(=-0.434,=0.033)。与后狭窄去氧相关的高氧相关的去氧伴随区域性舒张应变率降低(1.39±0.57 对 1.18±0.65;=0.045)和收缩径向速度降低(37.40±17.22 对 32.88±13.58;=0.038)。在室气中 T2 增加、心指数增加和定义的应变参数异常是高氧诱导异常的预测因素(<0.05)。此外,在固有 T1 延长(>1220 ms)的患者中,高氧降低射血分数和峰值应变。
对高氧挑战有应变异常的 CAD 和已有心肌损伤的患者似乎容易发生局部去氧和心肌功能恶化。